
The reasonable man adapts himself to the world; the unreasonable one persists in trying to adapt the world to himself. Therefore, all progress depends on the unreasonable man. GB Shaw
Wednesday, May 23, 2012
HROs
Tweeted by @peterlachman who is attending Risky Business, a link to a v useful resource about high reliability organizations. See here.
Tuesday, May 22, 2012
Waste and overuse
I read this paper recently and then reread it (subscription probably required); this I think is destined to become a classic. It touches on subject matter to which I have alluded in recent posts, Quality is goodness, Choosing Wisely and Waste and healthcare costs. The authors set out to examine the extent to which overuse of healthcare resources, defined as inappropriate diagnostics, treatments and medications has been studied. The results were striking in a very negative sense. Medline was searched for a period of 21 years, and a total of 172 papers were found which examined some aspect of overuse:
"We identified 172 articles measuring overuse: 53 concerned therapeutic procedures; 38, diagnostic tests; and 81, medications. Eighteen unique therapeutic procedures and 24 diagnostic services were evaluated, including 10 preventive diagnostic services. The most commonly studied services were antibiotics for upper respiratory tract infections (59 studies), coronary angiography (17 studies), carotid endarterectomy (13 studies), and coronary artery bypass grafting (10 studies)"In other words, 172 papers have sought to determine the extent of waste attributable to overuse (in the US healthcare system) out of >114,000 evaluated. Just to re-emphasise, some authorities estimate that waste contributes to 20-30% of US healthcare expenditure and we appear not to have even begun to systematically examine the extent of the problem. Even where the work has been done, it appears the papers are limited to a few main areas, including angiography, CABG, cartotid endartectomy, antibiotics for respiratory infections etc. Not that it is an easy thing to study, but surely government funding agencies should be in these challenging times insisting that more efforts be put into studying these areas rather than focussing on the next addition to our medical arsenal.
Monday, May 21, 2012
A Note to My Younger Colleagues. . .Be Brave
I was searching for a couple of papers by Harlan Krumholz today for another post and came across this piece just published. I found it inspiring. He writes about the difficulties and challenges of standing against the status quo, even when, especially when the vested interests as they mass in opposition seem to brook or tolerate no opposition. A few choice passages (underlined by me):
"Unfortunately, our profession does not often reward those who question dogma. In fact, there are many episodes throughout the history of medicine and science in which truth was resisted and dogmatic beliefs, however poorly supported by evidence, were imposed by those in a position to do so. If we are to accelerate innovation in medicine, eliminate waste- ful practices, and improve the depth and effectiveness of how we care for patients, then there must be room to question traditional approaches and to introduce new and better ways of prevention, diagnosis, and treatment. We are now at that critical juncture.
When I entered medicine, I did not realize that there was such intense pressure to conform. But we learn early on that there is a decorum to medicine, a politeness. A hidden curriculum teaches us not to disturb the status quo. We are trained to defer to authority, not to question it. We depend on powerful individuals and organizations and are taught that success does not often come to those who ask uncomfortable questions or suggest new ways of providing care.
I have grown to appreciate those who will stand up despite the risks or in the face of efforts to silence them. Promoting the best science and the best advocacy for patients and the public sometimes entails risk. Change does not come easily to a system and there is resistance to those who may seek to make the system safer, more effective, and more patient-centered through new ideas or the articulation of uncomfortable truths."He also quotes from Victor Montori, from Mayo Clinic who writes:
"I have struggled with this issue for years. Turns out that this is a common struggle for those who find themselves unable to stay silent in the face of waste, error, low integrity, or abuse.
If you find yourself with some time (not a lot), let me recommend Letters to a Young Contrarian by Hitchens.His argument that clarity emerges from conflict is compelling. And for conflict to emerge, ie for clarity to emerge, someone has to take a position. The question you ask is whether this should be you, now, and at this stage of your career."
Read it and distribute widely.
Sunday, May 20, 2012
Quality is goodness
In the spirit of stealing shamelessly, I am going to plunder Anna Roths latest post from her blog. She summarises a talk by Dr. Don Berwick. Highlights include:
"Quality is Goodness"
"What do we need to do? This is the 2.6 trillion dollar question isn't it? Here is a list to help guide us.
1. Put patients first
2. Protect the disadvantaged
3. Start at scale –move fast – go "all in"
4. Return the money
5. Act locally"
"The Ethics of Improvement
- Professionals have a duty to help improve the systems in which they work.
- Leaders have a duty to make 1. Logistical, feasible and supported.
- No excuses for inaction on 1 and 2 are acceptable.
- The duty to improve encompasses safety, efficiency, patient-centeredness, timeliness, effectiveness, and equity requires continual reduction of waste. The IOM six dimensions quality of are dimensions of goodness
- Those who educate professionals have the duty to prepare them for improvement work."
Wow, in 25 plus years of training, working, and teaching, no-one has ever said to me there is an ethical duty to educate professionals for improvement. Self evident but an indication of why we are finding healthcare improvement to be so challenging.
Anna is always worth reading. Follow her blog and twitter.
Friday, May 18, 2012
Economics of improving quality
There is a constant tension in healthcare between the economic/ financial imperatives and the clinical demands. Not unreasonably, based on healthcare inflation around the world over the last 40 years, there is a belief that more (which for many people, clinicians and patients) healthcare is better healthcare. Those of us interested in quality believe that this is not always the case. However the quality people I believe have been remiss in not addressing the evidence base for what they do, or the economic benefits of improving quality. Followers of Deming believe unequivocally that improving quality drives down cost. Brent James firmly believes that improving quality in Intermountain has not only improved care but dramatically driven down costs. Hence the importance of this paper just published and free to access.
The authors aim was to systematically review comparative economic analyses of patient safety improvements in the acute care setting and they explored 15 patient safety conditions and six associated improvement strategies. They concluded that pharmacist-led medication reconciliation, the Keystone ICU intervention for central line-associated bloodstream infections, chlorhexidine for vascular catheter site care, and standard surgical sponge counts were economically attractive strategies for improving patient safety.
Great stuff, a lot more needed.
The authors aim was to systematically review comparative economic analyses of patient safety improvements in the acute care setting and they explored 15 patient safety conditions and six associated improvement strategies. They concluded that pharmacist-led medication reconciliation, the Keystone ICU intervention for central line-associated bloodstream infections, chlorhexidine for vascular catheter site care, and standard surgical sponge counts were economically attractive strategies for improving patient safety.
Great stuff, a lot more needed.
Thursday, May 17, 2012
Choosing Wisely
A very interesting initiative has been undertaken by a large number of medical professional bodies in the US. Termed Choosing Wisely, 9 societies have each listed 5 procedures which they believe are overused, and which they feel need some consideration and discussion prior to being used. To learn more, check out IHI WIHI on May 17th which will discuss tis in more detail. As Churchill said about the US,
“You can always count on Americans to do the right thing - after they've tried everything else.”
Listen in, it;'s free and promises to provoke some thinking
“You can always count on Americans to do the right thing - after they've tried everything else.”
Listen in, it;'s free and promises to provoke some thinking
Child Protection & Professionals
Anyone with a passing knowledge of the David Southall saga probably shivers. A very comprehensive account has just bene published in the BMJ here, which will only add I think to the fear that many professionals, especially pediatricians have when faced with child protection cases. As the article says, quoting the esteemed editor of Pediatrics, Jerrold Lucey, “There is something grossly wrong with the medical and legal system which allowed this to happen."
Empathy robots
ZDogg MD is a genius, cant vouch for his medical expertise, but as a comedian, he has few competitors, (ok a bit of an exaggeration). Check this video out if you are having a bad day.
Wednesday, May 16, 2012
Gawande and 200 years of surgery
A wonderful piece of writing from Medicines prose laureate. This comes from the NEJM 200th anniversary series and Atul Gawande writes about the history of surgery. My favourite paragraph,
"It would take a little while for surgeons to discover that the use of anesthesia allowed them time to be meticulous. Despite the advantages of anesthesia, Liston, like many other surgeons, proceeded in his usual lightning-quick and bloody way. Spectators in the operating-theater gallery would still get out their pocket watches to time him. The butler's operation, for instance, took an astonishing 25 seconds from incision to wound closure. (Liston operated so fast that he once accidentally amputated an assistant's fingers along with a patient's leg, according to Hollingham. The patient and the assistant both died of sepsis, and a spectator reportedly died of shock, resulting in the only known procedure with a 300% mortality.)"
"It would take a little while for surgeons to discover that the use of anesthesia allowed them time to be meticulous. Despite the advantages of anesthesia, Liston, like many other surgeons, proceeded in his usual lightning-quick and bloody way. Spectators in the operating-theater gallery would still get out their pocket watches to time him. The butler's operation, for instance, took an astonishing 25 seconds from incision to wound closure. (Liston operated so fast that he once accidentally amputated an assistant's fingers along with a patient's leg, according to Hollingham. The patient and the assistant both died of sepsis, and a spectator reportedly died of shock, resulting in the only known procedure with a 300% mortality.)"
Tuesday, May 15, 2012
First contact with Deming
According to Charles Kenney in his book, "The Best Practice" Dr. Paul Batalden first became aware of Deming and his work when he read an article about him in the New York Times. As far as I can ascertain, the article is here, well worth a read. From Batalden, it appears the Deming gospel was spread to Dr. Berwick. From small acorns, great oaks grow. By the way, The Best practice is well worth a read for all you healthcare quality junkies out there.
Waste and healthcare costs
Dr Berwick has written two pieces in which he makes the case that waste broadly defined accounts for 20-30% of US healthcare expenditure. JAMA article requires subscription here and Boston Globe piece here.
He defines waste as follows:
He defines waste as follows:
- Over-treatment
- Failures of care coordination
- Failures in execution of care processes
- Administrative complexity
- Pricing failures, and
- Fraud and abuse
I can certainly see items 1-5 occurring in our system; whether fraud contributes a substantial amount, I just dont have the data. I am guessing failed IT implementation falls into category 4. Interestingly the Vanguard organisation has provided initial estimates based on preliminary work that what they term failure demand (which would certainly fit into category 1-4 above accounts for a very substantial proportion of healthcare activity), for an example see here.
Saturday, April 21, 2012
Interested in spreading QI?
A very useful resource, here, for anyone interested in implementing and spreading quality improvement in healthcare. Full of lessons learned and suggestion on overcoming barriers.
"they identified 10 key challenges to improvement that consistently emerged in the programmes evaluated:
- convincing people that there is a problem
- convincing people that the solution chosen is the right one
- getting data collection and monitoring systems right
- excess ambitions and ‘projectness’
- the organisational context, culture and capacities
- tribalism and lack of staff engagement
- leadership
- balancing carrots and sticks – harnessing commitment through incentives and potential sanctions
- securing sustainability
- considering the side effects of change.
Friday, January 27, 2012
Checklists Again.
If one wanted hard evidence that checklists are effective, read this piece in the New York Times about pharma companies using symptom checklists which allow potential patients to confirm their diagnosis which in turn may lead to the prescription of a drug made by that pharma company. Wonderful! Or maybe not?
Thursday, November 3, 2011
The system is dead, long live the system
If you believe, as I do, that the current model of Western healthcare delivery is dying, I suggest you read this piece. Medicine is succumbing to the disease that infects all large human endeavors, the current structures seek to justify and build upon themselves. Even if done for the best of reasons, the usual solution sought from heath care workers is to build more of the same, buy more of the same, do more of the same. I see many parallels between the military industrial complex that worried Eisenhower, and our current medical industrial complex.
Tuesday, October 18, 2011
Escape Fire and high reliability
I have bene rereading two books recently, Managing the Unexpected, (a fantastic read) and Berwicks Escape Fire. Berwick spoke about the Mann gulch fire disaster in Montana, about which Weick has written. Although at first pass, one wonders what lessons a forest fire in Montana has to delivering safe care in health, there are many deep lessons to be learned. This is a paper well worth reading. A few examples.
Partners and partnership are critical.
To be wise is not to know particular facts but to know without excessive confidence or excessive cautiousness. Wisdom is thus not a belief, a value, a set of facts, a corpus of knowledge or information in some specialized area, or a set of special abilities or skills. Wisdom is an attitude taken by persons toward the beliefs, values, knowledge, information, abilities, and skills that are held, a tendency to doubt that these are necessarily true or valid and to doubt that they are an exhaustive set of those things that could be known.
In a fluid world, wise people know that they don't fully understand what is happening right now, because they have never seen precisely this event before. Extreme confidence and extreme caution both can destroy what organizations most need in changing times, namely, curiosity, openness, and complex sensing. The overconfident shun curiosity because they feel they know most of what there is to know. The overcautious shun curiosity for fear it will only deepen their uncertainties. Both the cautious and the confident are closed-minded, which means neither makes good judgments. It is this sense in which wisdom, which avoids extremes, improves adaptability.
Partners and partnership are critical.
A partner makes social construction easier. A partner is a second source of ideas. A partner strengthens independent judgment in the face of a majority. And a partner enlarges the pool of data that are considered. Partnerships that endure are likely to be those that adhere to Campbell's three imperatives for social life, based on a reanalysis of Asch's (1952) conformity experiment:
(1) Respect the reports of others and be willing to base beliefs and actions on them (trust);
(2) Report honestly so that others may use your observations in coming to valid beliefs (honesty); and,
(3) Respect your own perceptions and beliefs and seek to integrate them with the reports of others without deprecating them or yourselves (self-respect).
Wednesday, October 12, 2011
Motivation and work satisfaction.
Reading Quality by Design; well worth delving into. A quote by Paul O'Neill, ex CEO of Alcoa and Former Secretary of the US Treasury.
"I am treated with dignity and respect everyday by everyone i encounter... and it doesn't have anything to do with hierarchy. I'm given the opportunity and the tools that i need to make a contribution and this gives meaning to my life. Someone noticed that I did it.O'Neill states that a high level of work-life satisfaction exists when every employee can strongly agree with these three statements. A simple approach, too often disregarded in health organisations.
Monday, October 10, 2011
Disruptive Innovation
From one of my fave blogs, The Big Picture, comes a great graphic about disruptive innovation. Bottom line;
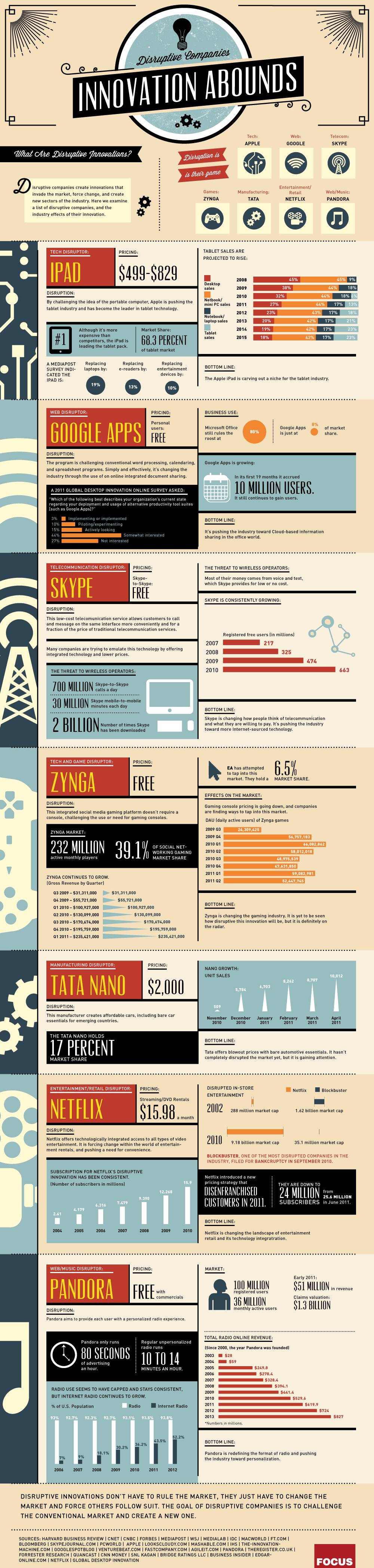{kind=link}
Disruptive innovations don't have to rule the market, they just have to change the market and force others to follow suit. The goal of disruptive companies is to challenge the conventional market and create a new one.
Monday, October 3, 2011
Improve patient experience and staff experience
I read a few days ago two articles in BMJ Quality and Safety, (here and here, sorry sub required) in which patients recounted their experiences, (pretty bad). A letter in response makes the point that addressing the defects that result in poor care not only improves the patient experience, but also makes work more satisfying for staff. A true win-win.
"Frontline staff frequently struggle with infrastructure issues that inhibit their ability to deliver high quality care, undermine their work flow and also affect their morale. Many of these same infrastructure problems frustrate patients as much as they do staff. Some patient safety problems thus represent a win–win situation from an organisation's point of view: addressing them improves patient safety and increases the efficiency of frontline staff, as well as the quality of their work life."
Safety in Primary Care
Safety in hospital care (or the lack of) gets the lions share of attention. However, little is known about safety in primary care; even if substantially safer, there may still be substantial risks given the huge numbers who access care through their GP as compared to the numbers accessing hospital services. A piece that discussed this subject is published here by BMJ.
"Do we really know how safe general practice is? And where we identify problems, what sort of mechanisms do we have to ensure that the sort of poor practice that the programme identified is addressed? "
Sunday, October 2, 2011
ZDOGG
I must admit, I love ZDOGG MD. This piece is a classic. Mental Illness on Sesame Street. Check it out, it will cheer your day.
Subscribe to:
Comments (Atom)