
The reasonable man adapts himself to the world; the unreasonable one persists in trying to adapt the world to himself. Therefore, all progress depends on the unreasonable man. GB Shaw
Thursday, November 3, 2011
The system is dead, long live the system
If you believe, as I do, that the current model of Western healthcare delivery is dying, I suggest you read this piece. Medicine is succumbing to the disease that infects all large human endeavors, the current structures seek to justify and build upon themselves. Even if done for the best of reasons, the usual solution sought from heath care workers is to build more of the same, buy more of the same, do more of the same. I see many parallels between the military industrial complex that worried Eisenhower, and our current medical industrial complex.
Tuesday, October 18, 2011
Escape Fire and high reliability
I have bene rereading two books recently, Managing the Unexpected, (a fantastic read) and Berwicks Escape Fire. Berwick spoke about the Mann gulch fire disaster in Montana, about which Weick has written. Although at first pass, one wonders what lessons a forest fire in Montana has to delivering safe care in health, there are many deep lessons to be learned. This is a paper well worth reading. A few examples.
Partners and partnership are critical.
To be wise is not to know particular facts but to know without excessive confidence or excessive cautiousness. Wisdom is thus not a belief, a value, a set of facts, a corpus of knowledge or information in some specialized area, or a set of special abilities or skills. Wisdom is an attitude taken by persons toward the beliefs, values, knowledge, information, abilities, and skills that are held, a tendency to doubt that these are necessarily true or valid and to doubt that they are an exhaustive set of those things that could be known.
In a fluid world, wise people know that they don't fully understand what is happening right now, because they have never seen precisely this event before. Extreme confidence and extreme caution both can destroy what organizations most need in changing times, namely, curiosity, openness, and complex sensing. The overconfident shun curiosity because they feel they know most of what there is to know. The overcautious shun curiosity for fear it will only deepen their uncertainties. Both the cautious and the confident are closed-minded, which means neither makes good judgments. It is this sense in which wisdom, which avoids extremes, improves adaptability.
Partners and partnership are critical.
A partner makes social construction easier. A partner is a second source of ideas. A partner strengthens independent judgment in the face of a majority. And a partner enlarges the pool of data that are considered. Partnerships that endure are likely to be those that adhere to Campbell's three imperatives for social life, based on a reanalysis of Asch's (1952) conformity experiment:
(1) Respect the reports of others and be willing to base beliefs and actions on them (trust);
(2) Report honestly so that others may use your observations in coming to valid beliefs (honesty); and,
(3) Respect your own perceptions and beliefs and seek to integrate them with the reports of others without deprecating them or yourselves (self-respect).
Wednesday, October 12, 2011
Motivation and work satisfaction.
Reading Quality by Design; well worth delving into. A quote by Paul O'Neill, ex CEO of Alcoa and Former Secretary of the US Treasury.
"I am treated with dignity and respect everyday by everyone i encounter... and it doesn't have anything to do with hierarchy. I'm given the opportunity and the tools that i need to make a contribution and this gives meaning to my life. Someone noticed that I did it.O'Neill states that a high level of work-life satisfaction exists when every employee can strongly agree with these three statements. A simple approach, too often disregarded in health organisations.
Monday, October 10, 2011
Disruptive Innovation
From one of my fave blogs, The Big Picture, comes a great graphic about disruptive innovation. Bottom line;
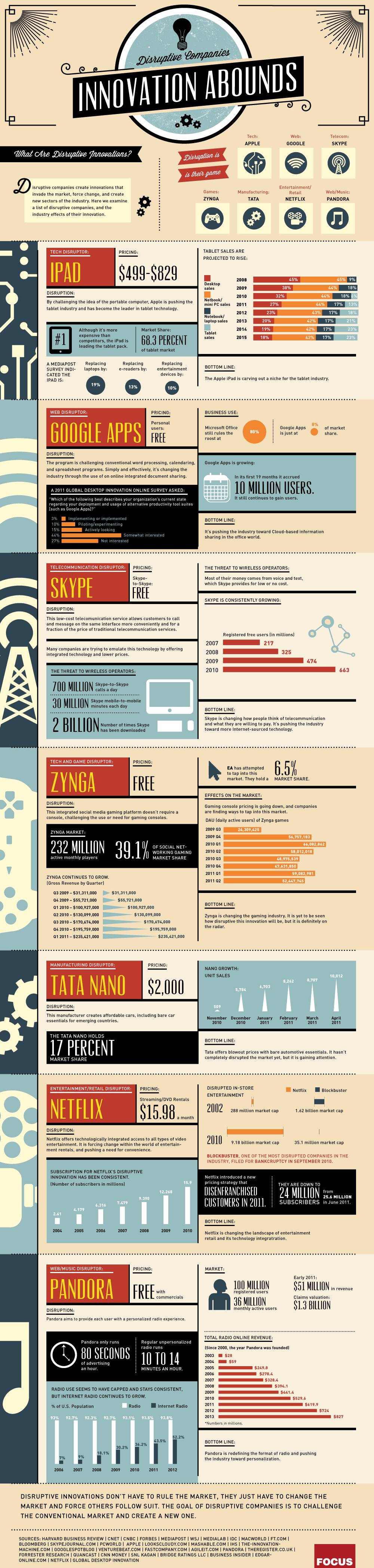{kind=link}
Disruptive innovations don't have to rule the market, they just have to change the market and force others to follow suit. The goal of disruptive companies is to challenge the conventional market and create a new one.
Monday, October 3, 2011
Improve patient experience and staff experience
I read a few days ago two articles in BMJ Quality and Safety, (here and here, sorry sub required) in which patients recounted their experiences, (pretty bad). A letter in response makes the point that addressing the defects that result in poor care not only improves the patient experience, but also makes work more satisfying for staff. A true win-win.
"Frontline staff frequently struggle with infrastructure issues that inhibit their ability to deliver high quality care, undermine their work flow and also affect their morale. Many of these same infrastructure problems frustrate patients as much as they do staff. Some patient safety problems thus represent a win–win situation from an organisation's point of view: addressing them improves patient safety and increases the efficiency of frontline staff, as well as the quality of their work life."
Safety in Primary Care
Safety in hospital care (or the lack of) gets the lions share of attention. However, little is known about safety in primary care; even if substantially safer, there may still be substantial risks given the huge numbers who access care through their GP as compared to the numbers accessing hospital services. A piece that discussed this subject is published here by BMJ.
"Do we really know how safe general practice is? And where we identify problems, what sort of mechanisms do we have to ensure that the sort of poor practice that the programme identified is addressed? "
Sunday, October 2, 2011
ZDOGG
I must admit, I love ZDOGG MD. This piece is a classic. Mental Illness on Sesame Street. Check it out, it will cheer your day.
Whistleblowing
I hate the term "whistleblower". It has all sorts of negative connotations, for doing something that is intended to stop bad behaviour, bad practice, and harm. At a meeting in London two years ago, i heard 3 "whistleblowers", all non-medical talk about their experience. they found it very harrowing, and i seem to recall all three saying they would never do it again. See here for a link to one of the speakers. Just a few days ago, I came across this piece, the story of the anesthetist who raised concerns about poor outcomes in children and babies undergoing heart surgery in Bristol.
A damning indictment.
Leaving the UK with my wife and family was an incredibly sad and disappointing time but I am sure now that there could never have been ‘Clinical Governance’ or a change in medical attitudes while I remained in the UK. Only when I had a contract in a new hospital, in a new country did I feel secure enough to report the mortality rate in the Bristol paediatric cardiac surgery unit to the GMC. Sadly despite the Presidents and Council Members of 2 Royal Colleges, the Dean of the Medical School, numerous Professors, some members of the Trust Board, members of the Department of Health and many local clinicians all knowing about Bristol, no other doctors in the UK reported these events to the GMC. I believe that this is a serious and permanent indictment of the attitudes of the profession that prevailed at that time and persist in some quarters in the UK. At least 12 sets of parents had reported deaths to the GMC, but their complaints would not have been investigated without a complaint from a doctor.
A damning indictment.
Friday, September 30, 2011
Risky Business
A report has just been published by the Royal College of Surgeons of England entitled “The Higher Risk General Surgical Patient: towards improved care for a forgotten group”. It is a very sobering examination of the outcome in non cardiac emergency surgery.
My pet interest of variation in care and outcomes is addressed.
Higher risk non-cardiac general surgery is undertaken in every acute hospital. By way of comparison, the mortality for this group, which includes most major gastro-intestinal and vascular procedures, exceeds that for cardiac surgery by two to three fold and complication rates of 50% are not uncommon. There may be a lack of awareness of the level of risk. Among these patients, emergency surgery and unscheduled management of complications is common and this group of patients are one of the largest consumers of critical care resources. The health and financial costs are considerable.The most amazing statistic in this paper is the fact that “Complications occur in as many as 50% of patients undergoing some common procedures.”
My pet interest of variation in care and outcomes is addressed.
Review of 2008/9 hospital episode statistics (HES) data from Dr Foster reveal a greater than two-fold variation in relative risk of 30-day mortality (risk-adjusted) after non-elective lower GI procedures between trusts in the North West SHA (strategic health authority). It is known that the chance of a patient dying in a UK hospital is 10% higher if he or she is admitted at a weekend rather than during the week.Anyone involved in ensuring good outcomes for surgical patients, or ensuring that hospital resources are used efficiently, (by reducing unnecessary complications) needs to read this.
Thursday, September 29, 2011
Normalisation of Deviance
One of my favourite terms is the “Normalisation of Deviance”. I think it captures perfectly what happens every day in healthcare. We work around problems, pat ourselves on the back for finding a (temporary) solution, and ignore the very profound message that the system is sending us; this message essentially is “you dont understand your system and your processes and if you dont work out a way to fix this problem, there will be serious consequences”. In Reasons Swiss Cheese model, all those little holes are problems that usually were recognised well before a serious event occured, but were most often ignored and certainly never consciously addressed and removed.
As Scott Snook, a lecturer from Harvard puts it:
As Scott Snook, a lecturer from Harvard puts it:
Each uneventful day that passes reinforces a steadily growing false sense of confidence that everything is all right – that I, we, my group must be OK because the way we did things today resulted in no adverse consequences.A paper that describes the consequences of this thinking, really a form of magical thinking is available on the NASA website; it is a section of the report into the Columbia Space Shuttle disaster. Available here.
Deming, why now?
A piece worth reading, published by the Deming Collaboration, and authored by Rafael Agauyo, who studied with Deming and subsequently published a book about Deming and his methods, (which is an excellent overview). Although there is a danger of assuming that one persons hero is the answer to all the worlds problems, Deming has outlined a systematic approach; contrast this with the toolbox approach, i.e. lets introduce lean or TQM or some other method de jour, stand back and watch our performance improve. Although Deming is probably best known for his PDSA, or PDCA cycle, his more profound contribution was the System of Profound Knowledge.
Coaching
A great and as ever thought provoking piece from Gawande. He discussed the value of coaching and describes his experience and initial results of using a surgical coach. Well worth a read.
Wednesday, September 28, 2011
Hard Jobs
A quote attributed to Peter Drucker, one of the great management gurus:
I find that hard to believe, but on mature reflection, maybe not.
- “The four hardest jobs in America (not necessarily in order) are: President of the United States, a university president, a hospital CEO, and a pastor.”
- “Health care is the most difficult, chaotic, and complex industry to manage today.”
- “The hospital is altogether the most complex human organization ever devised.”
Thursday, September 15, 2011
Physician Burnout
Physician burnout is a well recognised problem, and may be associated with other undesirable factors including substance abuse, depression, physician suicide and poor patient outcomes. I am seeing the phenomenon of burnout more frequently, but my impression is that the response of the system is not just to ignore this but to continue to pile on more pressure.
A paper just published here reports some very disturbing findings.
A paper just published here reports some very disturbing findings.
Quality of life was rated “as bad as it can be” or “somewhat bad” by 2402 of 16 187 responding residents (14.8%). Overall burnout and high levels of emotional exhaustion and depersonalization were reported by 8343 of 16 192 (51.5%), 7394 of 16 154 (45.8%), and 4541 of 15 737 (28.9%) responding residents, respectively.Interestingly, international medical graduates showed lower levels of distress. The fundamental problem in my view is that physicians refuse to recognize these problems in their colleagues and indeed see such problems as “weakness and failure”
One factor in the difficulty in ensuring change happens in healthcare is that healthcare workers, especially doctors, find it easy to work around the system. If we had to wait as long as our patients, perhaps we might be more enthusiastic about changing and leading the change that must happen in our systems. A recent report suggests that our ability to circumvent the system, at least in the US is associated with a higher prevalence of disease than would be expected in the population; in other words does the ease of access imply an ease of diagnosis. Having had a recent experience of healthcare, it does appear to me that at least for doctors, other doctors may be more likely to test and treat.
Mirror, Mirror on the wall, who is the best of us all?
Conventional wisdom suggest that bigger and more sophisticated hospitals offer the best care. However, my anecdotal experience suggest that this may not always be the case. There are some emerging data which also put the lie to this hypothesis. Just published is The Joint Commissions annual survey of hospital quality in the US.
The measures used to assess quality might be criticized as “process“ measures, i.e. Are we delivering the care that we are supposed to deliver? but these are basic widely agreed measures. The most stunning finding was that many of the big name hospitals, even those that have tried to make their name as institutions that prioritize quality and safe care do not feature. Or maybe not so surprising; in a culture in which individuals prize their autonomy, it will be easier for smaller hospitals to ensure they are consistent in applying processes.
The measures used to assess quality might be criticized as “process“ measures, i.e. Are we delivering the care that we are supposed to deliver? but these are basic widely agreed measures. The most stunning finding was that many of the big name hospitals, even those that have tried to make their name as institutions that prioritize quality and safe care do not feature. Or maybe not so surprising; in a culture in which individuals prize their autonomy, it will be easier for smaller hospitals to ensure they are consistent in applying processes.
Wednesday, September 7, 2011
Competition?
Competition is touted as a solution for all the ills that afflict healthcare, not withstanding the evidence from a market that is not deficient in competition, the US, that more competition does not equate to better healthcare. One of the great thinkers, Muir Gray, has written two recent blog posts, here and here, which outline a pragmatic framework which could be used to foster improved healthcare. Strongly recommended reading.
Systems Thinking in the Public Sector
I have previously written about Vanguard, John Seddon and his approach to systems thinking. His writing has been a revelation to me, plainly explaining how we can do things better with fewer resources, less waste, more customer satisfaction and more job satisfaction. Not quite a free lunch, but the next best thing. See the Amazon link on the side panel. I strongly recommend his books.
How to measure harm
Amongst the many challenges we face in trying to improve safety of care is the paucity of knowledge we possess about the rate and types of harm occurring to our patients. The traditional approach has been to identify sentinel cases, either because they are obvious or they are reported via traditional risk reporting structures. This approach has many limitations. A more recent approach has been to systematically review charts looking for evidence of adverse events, which allows one to both measure the rate of harm, identify areas of greatest risk and then one can determine whether changes made are having any meaningful effect in reducing rates of harm.
A paper just published (free here) describes an alternative approach in which a trained observer directly measures rates and type of harm occurring. The authors found almost 14% of patients suffered at least one adverse event, and 6% of all patients suffered a preventable adverse event. Overall 33% of adverse events were judged to be preventable. The rate of harm varied widely by specialty with <2% of obstetric patients being harmed to 11% of medical and ICU patients being harmed. The severity of harm also varied, with almost 5% of cardiac ICU patients dying or being permanently disabled due to an AE.
A paper just published (free here) describes an alternative approach in which a trained observer directly measures rates and type of harm occurring. The authors found almost 14% of patients suffered at least one adverse event, and 6% of all patients suffered a preventable adverse event. Overall 33% of adverse events were judged to be preventable. The rate of harm varied widely by specialty with <2% of obstetric patients being harmed to 11% of medical and ICU patients being harmed. The severity of harm also varied, with almost 5% of cardiac ICU patients dying or being permanently disabled due to an AE.
Subscribe to:
Posts (Atom)