
The reasonable man adapts himself to the world; the unreasonable one persists in trying to adapt the world to himself. Therefore, all progress depends on the unreasonable man. GB Shaw
Thursday, November 3, 2011
The system is dead, long live the system
If you believe, as I do, that the current model of Western healthcare delivery is dying, I suggest you read this piece. Medicine is succumbing to the disease that infects all large human endeavors, the current structures seek to justify and build upon themselves. Even if done for the best of reasons, the usual solution sought from heath care workers is to build more of the same, buy more of the same, do more of the same. I see many parallels between the military industrial complex that worried Eisenhower, and our current medical industrial complex.
Tuesday, October 18, 2011
Escape Fire and high reliability
I have bene rereading two books recently, Managing the Unexpected, (a fantastic read) and Berwicks Escape Fire. Berwick spoke about the Mann gulch fire disaster in Montana, about which Weick has written. Although at first pass, one wonders what lessons a forest fire in Montana has to delivering safe care in health, there are many deep lessons to be learned. This is a paper well worth reading. A few examples.
Partners and partnership are critical.
To be wise is not to know particular facts but to know without excessive confidence or excessive cautiousness. Wisdom is thus not a belief, a value, a set of facts, a corpus of knowledge or information in some specialized area, or a set of special abilities or skills. Wisdom is an attitude taken by persons toward the beliefs, values, knowledge, information, abilities, and skills that are held, a tendency to doubt that these are necessarily true or valid and to doubt that they are an exhaustive set of those things that could be known.
In a fluid world, wise people know that they don't fully understand what is happening right now, because they have never seen precisely this event before. Extreme confidence and extreme caution both can destroy what organizations most need in changing times, namely, curiosity, openness, and complex sensing. The overconfident shun curiosity because they feel they know most of what there is to know. The overcautious shun curiosity for fear it will only deepen their uncertainties. Both the cautious and the confident are closed-minded, which means neither makes good judgments. It is this sense in which wisdom, which avoids extremes, improves adaptability.
Partners and partnership are critical.
A partner makes social construction easier. A partner is a second source of ideas. A partner strengthens independent judgment in the face of a majority. And a partner enlarges the pool of data that are considered. Partnerships that endure are likely to be those that adhere to Campbell's three imperatives for social life, based on a reanalysis of Asch's (1952) conformity experiment:
(1) Respect the reports of others and be willing to base beliefs and actions on them (trust);
(2) Report honestly so that others may use your observations in coming to valid beliefs (honesty); and,
(3) Respect your own perceptions and beliefs and seek to integrate them with the reports of others without deprecating them or yourselves (self-respect).
Wednesday, October 12, 2011
Motivation and work satisfaction.
Reading Quality by Design; well worth delving into. A quote by Paul O'Neill, ex CEO of Alcoa and Former Secretary of the US Treasury.
"I am treated with dignity and respect everyday by everyone i encounter... and it doesn't have anything to do with hierarchy. I'm given the opportunity and the tools that i need to make a contribution and this gives meaning to my life. Someone noticed that I did it.O'Neill states that a high level of work-life satisfaction exists when every employee can strongly agree with these three statements. A simple approach, too often disregarded in health organisations.
Monday, October 10, 2011
Disruptive Innovation
From one of my fave blogs, The Big Picture, comes a great graphic about disruptive innovation. Bottom line;
Disruptive innovations don't have to rule the market, they just have to change the market and force others to follow suit. The goal of disruptive companies is to challenge the conventional market and create a new one.
Monday, October 3, 2011
Improve patient experience and staff experience
I read a few days ago two articles in BMJ Quality and Safety, (here and here, sorry sub required) in which patients recounted their experiences, (pretty bad). A letter in response makes the point that addressing the defects that result in poor care not only improves the patient experience, but also makes work more satisfying for staff. A true win-win.
"Frontline staff frequently struggle with infrastructure issues that inhibit their ability to deliver high quality care, undermine their work flow and also affect their morale. Many of these same infrastructure problems frustrate patients as much as they do staff. Some patient safety problems thus represent a win–win situation from an organisation's point of view: addressing them improves patient safety and increases the efficiency of frontline staff, as well as the quality of their work life."
Safety in Primary Care
Safety in hospital care (or the lack of) gets the lions share of attention. However, little is known about safety in primary care; even if substantially safer, there may still be substantial risks given the huge numbers who access care through their GP as compared to the numbers accessing hospital services. A piece that discussed this subject is published here by BMJ.
"Do we really know how safe general practice is? And where we identify problems, what sort of mechanisms do we have to ensure that the sort of poor practice that the programme identified is addressed? "
Sunday, October 2, 2011
ZDOGG
I must admit, I love ZDOGG MD. This piece is a classic. Mental Illness on Sesame Street. Check it out, it will cheer your day.
Whistleblowing
I hate the term "whistleblower". It has all sorts of negative connotations, for doing something that is intended to stop bad behaviour, bad practice, and harm. At a meeting in London two years ago, i heard 3 "whistleblowers", all non-medical talk about their experience. they found it very harrowing, and i seem to recall all three saying they would never do it again. See here for a link to one of the speakers. Just a few days ago, I came across this piece, the story of the anesthetist who raised concerns about poor outcomes in children and babies undergoing heart surgery in Bristol.
A damning indictment.
Leaving the UK with my wife and family was an incredibly sad and disappointing time but I am sure now that there could never have been ‘Clinical Governance’ or a change in medical attitudes while I remained in the UK. Only when I had a contract in a new hospital, in a new country did I feel secure enough to report the mortality rate in the Bristol paediatric cardiac surgery unit to the GMC. Sadly despite the Presidents and Council Members of 2 Royal Colleges, the Dean of the Medical School, numerous Professors, some members of the Trust Board, members of the Department of Health and many local clinicians all knowing about Bristol, no other doctors in the UK reported these events to the GMC. I believe that this is a serious and permanent indictment of the attitudes of the profession that prevailed at that time and persist in some quarters in the UK. At least 12 sets of parents had reported deaths to the GMC, but their complaints would not have been investigated without a complaint from a doctor.
A damning indictment.
Friday, September 30, 2011
Risky Business
A report has just been published by the Royal College of Surgeons of England entitled “The Higher Risk General Surgical Patient: towards improved care for a forgotten group”. It is a very sobering examination of the outcome in non cardiac emergency surgery.
My pet interest of variation in care and outcomes is addressed.
Higher risk non-cardiac general surgery is undertaken in every acute hospital. By way of comparison, the mortality for this group, which includes most major gastro-intestinal and vascular procedures, exceeds that for cardiac surgery by two to three fold and complication rates of 50% are not uncommon. There may be a lack of awareness of the level of risk. Among these patients, emergency surgery and unscheduled management of complications is common and this group of patients are one of the largest consumers of critical care resources. The health and financial costs are considerable.The most amazing statistic in this paper is the fact that “Complications occur in as many as 50% of patients undergoing some common procedures.”
My pet interest of variation in care and outcomes is addressed.
Review of 2008/9 hospital episode statistics (HES) data from Dr Foster reveal a greater than two-fold variation in relative risk of 30-day mortality (risk-adjusted) after non-elective lower GI procedures between trusts in the North West SHA (strategic health authority). It is known that the chance of a patient dying in a UK hospital is 10% higher if he or she is admitted at a weekend rather than during the week.Anyone involved in ensuring good outcomes for surgical patients, or ensuring that hospital resources are used efficiently, (by reducing unnecessary complications) needs to read this.
Thursday, September 29, 2011
Normalisation of Deviance
One of my favourite terms is the “Normalisation of Deviance”. I think it captures perfectly what happens every day in healthcare. We work around problems, pat ourselves on the back for finding a (temporary) solution, and ignore the very profound message that the system is sending us; this message essentially is “you dont understand your system and your processes and if you dont work out a way to fix this problem, there will be serious consequences”. In Reasons Swiss Cheese model, all those little holes are problems that usually were recognised well before a serious event occured, but were most often ignored and certainly never consciously addressed and removed.
As Scott Snook, a lecturer from Harvard puts it:
As Scott Snook, a lecturer from Harvard puts it:
Each uneventful day that passes reinforces a steadily growing false sense of confidence that everything is all right – that I, we, my group must be OK because the way we did things today resulted in no adverse consequences.A paper that describes the consequences of this thinking, really a form of magical thinking is available on the NASA website; it is a section of the report into the Columbia Space Shuttle disaster. Available here.
Deming, why now?
A piece worth reading, published by the Deming Collaboration, and authored by Rafael Agauyo, who studied with Deming and subsequently published a book about Deming and his methods, (which is an excellent overview). Although there is a danger of assuming that one persons hero is the answer to all the worlds problems, Deming has outlined a systematic approach; contrast this with the toolbox approach, i.e. lets introduce lean or TQM or some other method de jour, stand back and watch our performance improve. Although Deming is probably best known for his PDSA, or PDCA cycle, his more profound contribution was the System of Profound Knowledge.
Coaching
A great and as ever thought provoking piece from Gawande. He discussed the value of coaching and describes his experience and initial results of using a surgical coach. Well worth a read.
Wednesday, September 28, 2011
Hard Jobs
A quote attributed to Peter Drucker, one of the great management gurus:
I find that hard to believe, but on mature reflection, maybe not.
- “The four hardest jobs in America (not necessarily in order) are: President of the United States, a university president, a hospital CEO, and a pastor.”
- “Health care is the most difficult, chaotic, and complex industry to manage today.”
- “The hospital is altogether the most complex human organization ever devised.”
Thursday, September 15, 2011
Physician Burnout
Physician burnout is a well recognised problem, and may be associated with other undesirable factors including substance abuse, depression, physician suicide and poor patient outcomes. I am seeing the phenomenon of burnout more frequently, but my impression is that the response of the system is not just to ignore this but to continue to pile on more pressure.
A paper just published here reports some very disturbing findings.
A paper just published here reports some very disturbing findings.
Quality of life was rated “as bad as it can be” or “somewhat bad” by 2402 of 16 187 responding residents (14.8%). Overall burnout and high levels of emotional exhaustion and depersonalization were reported by 8343 of 16 192 (51.5%), 7394 of 16 154 (45.8%), and 4541 of 15 737 (28.9%) responding residents, respectively.Interestingly, international medical graduates showed lower levels of distress. The fundamental problem in my view is that physicians refuse to recognize these problems in their colleagues and indeed see such problems as “weakness and failure”
One factor in the difficulty in ensuring change happens in healthcare is that healthcare workers, especially doctors, find it easy to work around the system. If we had to wait as long as our patients, perhaps we might be more enthusiastic about changing and leading the change that must happen in our systems. A recent report suggests that our ability to circumvent the system, at least in the US is associated with a higher prevalence of disease than would be expected in the population; in other words does the ease of access imply an ease of diagnosis. Having had a recent experience of healthcare, it does appear to me that at least for doctors, other doctors may be more likely to test and treat.
Mirror, Mirror on the wall, who is the best of us all?
Conventional wisdom suggest that bigger and more sophisticated hospitals offer the best care. However, my anecdotal experience suggest that this may not always be the case. There are some emerging data which also put the lie to this hypothesis. Just published is The Joint Commissions annual survey of hospital quality in the US.
The measures used to assess quality might be criticized as “process“ measures, i.e. Are we delivering the care that we are supposed to deliver? but these are basic widely agreed measures. The most stunning finding was that many of the big name hospitals, even those that have tried to make their name as institutions that prioritize quality and safe care do not feature. Or maybe not so surprising; in a culture in which individuals prize their autonomy, it will be easier for smaller hospitals to ensure they are consistent in applying processes.
The measures used to assess quality might be criticized as “process“ measures, i.e. Are we delivering the care that we are supposed to deliver? but these are basic widely agreed measures. The most stunning finding was that many of the big name hospitals, even those that have tried to make their name as institutions that prioritize quality and safe care do not feature. Or maybe not so surprising; in a culture in which individuals prize their autonomy, it will be easier for smaller hospitals to ensure they are consistent in applying processes.
Wednesday, September 7, 2011
Competition?
Competition is touted as a solution for all the ills that afflict healthcare, not withstanding the evidence from a market that is not deficient in competition, the US, that more competition does not equate to better healthcare. One of the great thinkers, Muir Gray, has written two recent blog posts, here and here, which outline a pragmatic framework which could be used to foster improved healthcare. Strongly recommended reading.
Systems Thinking in the Public Sector
I have previously written about Vanguard, John Seddon and his approach to systems thinking. His writing has been a revelation to me, plainly explaining how we can do things better with fewer resources, less waste, more customer satisfaction and more job satisfaction. Not quite a free lunch, but the next best thing. See the Amazon link on the side panel. I strongly recommend his books.
How to measure harm
Amongst the many challenges we face in trying to improve safety of care is the paucity of knowledge we possess about the rate and types of harm occurring to our patients. The traditional approach has been to identify sentinel cases, either because they are obvious or they are reported via traditional risk reporting structures. This approach has many limitations. A more recent approach has been to systematically review charts looking for evidence of adverse events, which allows one to both measure the rate of harm, identify areas of greatest risk and then one can determine whether changes made are having any meaningful effect in reducing rates of harm.
A paper just published (free here) describes an alternative approach in which a trained observer directly measures rates and type of harm occurring. The authors found almost 14% of patients suffered at least one adverse event, and 6% of all patients suffered a preventable adverse event. Overall 33% of adverse events were judged to be preventable. The rate of harm varied widely by specialty with <2% of obstetric patients being harmed to 11% of medical and ICU patients being harmed. The severity of harm also varied, with almost 5% of cardiac ICU patients dying or being permanently disabled due to an AE.
A paper just published (free here) describes an alternative approach in which a trained observer directly measures rates and type of harm occurring. The authors found almost 14% of patients suffered at least one adverse event, and 6% of all patients suffered a preventable adverse event. Overall 33% of adverse events were judged to be preventable. The rate of harm varied widely by specialty with <2% of obstetric patients being harmed to 11% of medical and ICU patients being harmed. The severity of harm also varied, with almost 5% of cardiac ICU patients dying or being permanently disabled due to an AE.
Autumn and patient safety
After a long summer break, back to posting. I would strongly recommend this blog, authored by an Emergency Medicine physician, with a greta deal of expertise in the area of healthcare informatics. Well worth a read. http://frectal.com/
Friday, July 15, 2011
Systems Thinking in healthcare
This blog just launched is well worth checking out. Based on work by Vanguard, a UK systems thinking consultancy and its CEO, John Seddon. Seddons stuff, books, papers, podcasts etc are worth checking out. There is a simplicity which hides a very deep and profound complexity in his methods. I don't think they have done much in healthcare, but read Systems Thinking in the Public Sector , and you will immediately see analogies. Value Demand and Failure Demand have become part of my vernacular. Bottom line message, our healthcare system is broken, and we need to rethink it. Positive spin, there is a huge amount of waste. Read it and decide.
Thursday, July 14, 2011
Cowboys and Pit Crews
A great piece, as usual, from Gawande, with the aforementioned title. Bottom line, we have to change the way we think and work.
Tuesday, April 26, 2011

Sunday, April 24, 2011

Saturday, April 23, 2011

Thursday, April 21, 2011
Recession and Physical Child Abuse
A paper was presneted last week at the American Association of Neurological Surgeons' annual meeting in Denver by a fourth year medical student. Mary Huang presented her study which sought to determine whether there was an association between economic downturn and abusive head trauma in children. She found that the risk of abusive head trauma doubled during a economic recession, and the severity of the injuries appeared to increase also.
Wednesday, April 20, 2011
Patient Driven Care
A greta post on Paul Levys blog, in which he proclaims following a meeting in IHI that he is no longer an advocate for patient centered care, but henceforth will be proclaiming the benefits of patient driven care. In his own words,
"What I am suggesting is that clinicians should do their best to collaborate with patients to understand their needs and desires and to jointly design plans of care that are as consistent as possible with those needs and desires."
Such a move would require a sea change in the way we practice and deliver care. It reminds me of a good friend who when i told him the difficulty I was having in getting a computer in my clinic room asked me why I needed a computer. To access UpToDate and other resources, I replied. "You mean you would look up information in front of patients?", was the stunned response.
Pauls point aligns nicely with what Maureen Bisognano said at the International Forum, that patients are our greatest unused resource.
Sunday, April 17, 2011
Disclosure and Litigation
We are all aware of the reputation of the US legal system as litigation central for mistakes in healthcare. Surely the worst thing to do is to publicize ones mistakes in this environment? Paul Levy on his blog points out a fascinating cultural dichotomy. He explains how during his tenure as CEO of BIDMC, medical errors were publicized. He contrasts this openness with the reluctance of various European hospitals to disclose their errors. Perhaps we should be learning from our American cousins?
Lessons Learned
Just finished a book by a number of clinicians, all US based. It is outstanding. Written to honor Paul Batalden, it is a treasure chest of advice, hints, tips, aphorisms, about the practicalities of changing healthcare. Unusually I am unable to pick out a highlight, as the quality (no surprise) is uniformly excellent. Get it here.
Thursday, April 14, 2011
A vision of the future? Bilingual healthcare workers
From the inestimable Muir Gray, (thanks Tony), one possible approach to the problems facing us. Remember Einsteins definition of insanity, doing the same thing over and over and expecting different results. I think that summarizes healthcare. The model we have is designed, or rather evolved from the post war period to deal with a different set of problems. Acute self limited, or fatal illness. Coincident with the rise in healthcare technology, probably the early 50's with the development of ICUs following polio epidemics, the healthcare-industrial complex has in part generated problems and expectations that we are no longer equipped to handle. The paradigm of how care is delivered has to change radically. There is a very interesting book published in the 80's looking at how complex societies fail. The thesis and it applies equally well to complex systems is that a system evolves to deal with a complex problem, problems become more complex, hence the system becomes more complex and eventually a point of diminishing returns is reached where the inputs (think regulation, accreditation, legislation etc) consume more resources and the system collapses.
Gray provides one possible approach to this challenge. Basically the bilingualism to which he refers is that healthcare workers must be versed in not only the ability to provide clinical care to their patients,
"They need to know how to:
Gray provides one possible approach to this challenge. Basically the bilingualism to which he refers is that healthcare workers must be versed in not only the ability to provide clinical care to their patients,
"They need to know how to:
- Develop systems
- Build networks of clinicians and patients
- Design pathways
- Manage knowledge
- Harness the internet’s potential
- Engage patients
- Create and manage programme budgets
- Develop the right culture"
He describes this as population medicine. It is highly recommended.
Much ado about bundles
Following yesterdays post about bundles, a couple of interesting papers from this weeks NEJM. Two studies here and here, and an editorial about reducing infection in hospitals. The two studies came to different conclusions; the first examined the efficacy of screening for MRSA in ICUs and implementing barrier precautions on all patients until their MRSA status was known. The interventions were not shown to be effective in reducing transmission of MRSA or VRE. However, and this is the really big take home message for me, in cases where hand hygeine or glovers were indicated, the compliance with these measures was as low as 62%!
In contrast, the VA study instituted a bundle approach; a MRSA bundle was instituted in 2007 and over 2 million hospital discharges were studied. The rate of health care associated MRSA infections fell by between 45% (outside ICU) and 62% (inside ICU) over a two year period.
For some expert comment, see this CDC post.
In contrast, the VA study instituted a bundle approach; a MRSA bundle was instituted in 2007 and over 2 million hospital discharges were studied. The rate of health care associated MRSA infections fell by between 45% (outside ICU) and 62% (inside ICU) over a two year period.
For some expert comment, see this CDC post.
Is it better to be a dog or a medical student?
Lots doom and gloom out there, so something to put a smile on your face, unless you are a med student!
From A cartoon guide to becoming a doctor.

From A cartoon guide to becoming a doctor.
Wednesday, April 13, 2011
Health care spend, any room to reduce it?
While not strictly looking at quality and cost at a hospital level, a paper just published by OECD examines the potential for savings in health expenditure. It suggest that countries can achieve savings up to 5% of GNP by all countries becoming as efficient as the best performing countries. Note that there does not appear to be much if any correlation between healthcare spend and outcomes across countries. The authors suggest that countries by reaching the level of the best performers would increase life expectancy at birth by two years; in contrast a 10% rise in health expenditure would increase life expectancy by three to four months.
Harm
Great discussion by Bob Wachter on his blog about harm, preventable harm, errors and trigger tools amongst other things. He makes the point that we should focus on eliminating preventable harm, at least in the first instance. Beth Israel Deaconess publishes on its public website details on its progress towards eliminating preventable harm.
Giving doctors orders
If you are a doc, you know that very few people order you around, apart form your kids. Maureen Dowd discusses this and its implications in todays NYT. Yet another story of a family member dying. But she can be very amusing, and this is one of her funnier and more poignant pieces.
Bundles of joy or of sorrow?
The idea of bundles makes intuitive sense, gather together some evidence based interventions and ensure they are implemented reliably all the time, sit back and watch the magic. Pronovost showed the power of bundles in his NEJM paper some years ago. An observational study by Jarman and others in the BMJ last year suggested that using various bundles in a large London hospital was associated with a large reduction in hospital mortality.
So along come the surgeons to upset the consensus. A study in Archives of Surgery compared standard institutional practice with an extended bundle of interventions, all of which had been previously demonstrated in isolation to be effective. These interventions included:
So along come the surgeons to upset the consensus. A study in Archives of Surgery compared standard institutional practice with an extended bundle of interventions, all of which had been previously demonstrated in isolation to be effective. These interventions included:
- No pre-operative bowel preparation
- Pre-operative and intra-operative patient warming
- Supplemental oxygen intra and post operatively
- Intra-operative fluid restriction
- Use of a surgical wound protector
Any explanation? Its possible that the interventions are ineffective, or less likely that they are counter synergistic, i.e. although singly beneficial, when combined they counteract one another. Alternatively even positive studies may due to chance be negative. The main concern though apart from giving ammunition to those who wish to reject the benefits of standardisation is that there will be a call for more RCTs in this and every other areas. While we have traditionally believed that RCTs are the gold standard, Ioanniddis work is even questioning this dictum. The other big problem in conducting RCTs is that we assume that apart from the intervention being studied, all other factors are uniform. This is clearly not the case, and this has proven to be a difficult obstacle to surmount in trials of equipment such as new ventilators.
Game changing move for patient safety in US
Bob Wachter on THCB has a piece on what he calls a game changing safety initiative. Berwick and Kathleen Sibelius announced yesterday the "Partnership for Patients". This is a very ambitious well funded widely supported program. Its stated goals are to reduce preventable harm in US hospitals by 40% and preventable readmissions by 20% by 2013! It's nice to see Berwick has not lost his taste for aiming high. To quote Wachter:
Interestingly, the means of audit to confirm compliance with these aims will be a detailed chart which appears to me to be using the IHI global trigger tool. Exciting times.
It would appear in some ways to be modeled on the 100,000 Lives campaign in that it sets lofty goals, appeals to sentiment, has a short time frame and uses social pressure to ensure others want to join.
The financial stick is that by 2015, 9% of medicare reimbursement will be tied to reaching these goals.
- "For the first time, it establishes safety goals and programs as a private/public partnership, with early buy in from large insurers and employers. A broad tableau of leaders from provider organizations, insurers, federal agencies, businesses, and patient groups shared the stage with Sebelius and Berwick at this morning’s announcement to highlight the partnership theme.
- It provides large amounts of funding and technical assistance – nearly one billion dollars – both through the new CMS Innovation Center and elsewhere, to promote new knowledge and skill building.
- Like the 100K Lives Campaign, it seeks commitments from hospital executives and boards to tackle key safety goals.
- It provides support for collaborative networks designed to promote shared learning.
- It rewards hospitals for achieving certain milestones with both recognition and additional resources; those that do very well will be eligible to receive funding to help other hospitals improve."
Interestingly, the means of audit to confirm compliance with these aims will be a detailed chart which appears to me to be using the IHI global trigger tool. Exciting times.
It would appear in some ways to be modeled on the 100,000 Lives campaign in that it sets lofty goals, appeals to sentiment, has a short time frame and uses social pressure to ensure others want to join.
Tuesday, April 12, 2011
Innovation
A quote that came through in an IHI email today about innovation:
"Innovation distinguishes between a leader and a follower"
Steve Jobs
Not sure I totally agree. Many innovators failed to benefit from their innovations, and often the mindset of an innovator is antithetical to being a leader. Nevertheless, a great quote from the man who invented Peters iPad 2, (x2)
"Innovation distinguishes between a leader and a follower"
Steve Jobs
Not sure I totally agree. Many innovators failed to benefit from their innovations, and often the mindset of an innovator is antithetical to being a leader. Nevertheless, a great quote from the man who invented Peters iPad 2, (x2)
Depression, the inside story
Anyone interested in how our system within our own lifetimes treated people should read this article. It is harrowing. Unfortunately I think mental illness is still seen as a weakness, "just snap out of it, for gods sake" is often the response. I am aware of employers who have failed in their statutory responsibility to ensure those with mental illness receive the same entitlements and protections afforded to every employee. We are not as civilized as we think.
A quote from the psychiatrist who treated the patient:
A quote from the psychiatrist who treated the patient:
"Our patients are our best teachers. Jackie has taught me a huge amount about depression: what it feels like, the impact on sufferers’ and their family, and what does and doesn’t help.I have seen the toll taken by this ubiquitous disease, no less devastating in its impact than other chronic conditions. Jackie, an able and enthusiastic student, could barely finish her course at University, her employment prospects have been blighted, her social life restricted, and her capacity for pleasure and fulfilment curtailed. At their worst psychiatric services reinforce sufferers’ feelings of isolation and powerlessness."
Increase comfort in the face of uncertainty
IDEO are a very interesting design and innovation firm based in California, and have done a lot of work in this area with Kaiser Permanante. They have provided assistance to the NHS Institute for Innovation and Improvement, Texas Children's Paediatric Associates, (the largest primary paediatric care network in the US) and many others. Their website is well worth checking out for anyone with an interest in healthcare innovation in its softer (i.e. not hardware, expensive drugs and hi tech equipment) guise. What caught my eye recently was a blog by an IDEO employee with the title that I have posted above. I liked their use of data from Twitter, and Google Analytics to measure the "buzz" in real time generated by their ideas.
This comes back to the point made by Maureen Bisognano recently, about using the power of patients to seek ideas. If we could measure what people believe is important judged by what they search or discuss on line, perhaps it might help us focus on what matters to patients as opposed to what matters to the "providers". Just a thought.
This I think is an area where some Irish design consultancies might find a niche.
This comes back to the point made by Maureen Bisognano recently, about using the power of patients to seek ideas. If we could measure what people believe is important judged by what they search or discuss on line, perhaps it might help us focus on what matters to patients as opposed to what matters to the "providers". Just a thought.
This I think is an area where some Irish design consultancies might find a niche.
Monday, April 11, 2011

Global Trigger Tools
Thanks to Annette and Levette. Two important pieces to check out if you are interested in trigger tools. First a paper in Health Affairs showing that the use of the Global Trigger Tool detects adverse events at a rate 10 times greater than voluntary reporting or using the AHRQ patient safety indicators.
Second, an upcoming WIHI:
The Power to Detect and Improve: Revisiting the IHI Global Trigger Tool and Adverse Events
Thursday, April 14, 2011, 7pm MT. See here for details. Both are free. The WIHI features great faculty. Check it out.
Second, an upcoming WIHI:
The Power to Detect and Improve: Revisiting the IHI Global Trigger Tool and Adverse Events
Thursday, April 14, 2011, 7pm MT. See here for details. Both are free. The WIHI features great faculty. Check it out.
Mental illness and children
A great image showing the extent of psychoactive drug prescribing in the US. While there are many
interesting explanations for such rampant pharmaco-terrorism, this post has another purpose.
 A recent story caught my eye, in fact it was so striking it kidnapped my brain. Headlined, "Is that Thorazine in the babies bottle?", it discussed the relentless rise in diagnosing and treating psychiatric illness in chilren and infants. According to the story, 500,000 children in the US are prescribed anti-psychotics! When I went looking for data about the incidence/ prevalence of psychiatric illness in children, the numbers are mind boggling. According to childstats.gov, in 2008 8% of children aged 12-17 experienced a major depressive episode. Of course, some may question this data, but it does appear that the incidence of major psychiatric illness, especially depression is rising across the Western world, and it has been suggested that the major contributor to this increase is rising economic and social inequality. If this is the case, medicating children from a very young age is not the solution, and is really only addressing the symptoms of a societal problem. For a more detailed discussion, read The Spirit Level . This is a magnificent book, likely to be seen in 50 years as the seminal public health work.
A recent story caught my eye, in fact it was so striking it kidnapped my brain. Headlined, "Is that Thorazine in the babies bottle?", it discussed the relentless rise in diagnosing and treating psychiatric illness in chilren and infants. According to the story, 500,000 children in the US are prescribed anti-psychotics! When I went looking for data about the incidence/ prevalence of psychiatric illness in children, the numbers are mind boggling. According to childstats.gov, in 2008 8% of children aged 12-17 experienced a major depressive episode. Of course, some may question this data, but it does appear that the incidence of major psychiatric illness, especially depression is rising across the Western world, and it has been suggested that the major contributor to this increase is rising economic and social inequality. If this is the case, medicating children from a very young age is not the solution, and is really only addressing the symptoms of a societal problem. For a more detailed discussion, read The Spirit Level . This is a magnificent book, likely to be seen in 50 years as the seminal public health work.
interesting explanations for such rampant pharmaco-terrorism, this post has another purpose.
Saturday, April 9, 2011
Friday, April 8, 2011
International Forum and Social Movements
Helen Bevan and Maxine Power gave a wonderful hour long talk on the power of social movements, mobilising weak network connections, (in contrast to the network effects we usually think of being most powerful such as family, peers) in generating will to change. The focus was hospital based care, but I wonder how soon we will begin to see such strategies applied to the overwhelming need for society to concentrate on health and prevention.
Thursday, April 7, 2011

Forum; motivation and morale
Both Maureen Bisognano and Helen Bevan referenced the need to capture ant tap resources that we traditionally have failed to recognise. In Maureens case, the patient is a huge resource; Helen argues that we fail to capture the intrinsic motivation of many employees. The idea is that if an organisation can tap this, productivity can increase 30-40%.
international Forum and Maureen Bisognano and hospital flow
Maureen Bisognano in her keynote speech referenced specifically Eugene Litvaks work, and the benefits accrued to Cincinnati Childrens by implementing the methods he espouses. See my previous post about Litvaks work. http://saferhealthcareireland.blogspot.com/2011/03/optimizing-patient-flow-to-enhance.html
Emily Friedman at the International Forum
Magnificent keynote from Emily Friedman about challenges and possibilities for healthcare in Cambodia, harrowing stories. www.emilyfriedman.com
Wednesday, April 6, 2011

International Forum Quality Amsterdam
Outstanding plenary from Maureen Bisognano. talks about need to redefine healthcare leadership, both at a personal and sttructural level. Some interesting facts, medication compliance or lack of estimated to be 4th leading cause of death worldwide, accounts for >$150 billion in US health spend. Lots of opportunity to save, reduce waste, Gives various successful exemplars. Talks about need to refocus and suggests IHI Triple Aim as a useful model.
Tuesday, April 5, 2011
Quality Education
excellent piece from BMJ Q&S concerning education and training in healthcare quality and safety. The authors make a number of valid points.
There is a lack of suitably qualified experts in the area of health Quality and Safety to provide education
The traditional approach o education imposes an artificial barrier between clinical and improvement work; the two must be seen to be two sides of the same coin.
A consequence of this barrier is that front line staff fail to understand the true significance of quality improvement
This last point is one that has not previously occurred to me; the traditional method of teaching, asking questions, implies to the learner that every question and every problem has a solution, which is patently not the case.
The authors provide a framework to transform the way such training is delivered.
QI becomes an integral part of clinical practice and training
Students and teachers become co-learners, along with patients, families, and non clinical staff
QI is seen to result not from "great individuals", but from a team approach to problem solving
The end result is not judged by answering questions correctly, but how effectively a problem is solved.
There is a lack of suitably qualified experts in the area of health Quality and Safety to provide education
The traditional approach o education imposes an artificial barrier between clinical and improvement work; the two must be seen to be two sides of the same coin.
A consequence of this barrier is that front line staff fail to understand the true significance of quality improvement
This last point is one that has not previously occurred to me; the traditional method of teaching, asking questions, implies to the learner that every question and every problem has a solution, which is patently not the case.
The authors provide a framework to transform the way such training is delivered.
QI becomes an integral part of clinical practice and training
Students and teachers become co-learners, along with patients, families, and non clinical staff
QI is seen to result not from "great individuals", but from a team approach to problem solving
The end result is not judged by answering questions correctly, but how effectively a problem is solved.
Monday, April 4, 2011
Hot off the press
Just published, a supplement to BMJ Quality and safety, all open access, looks like some great stuff.
Tonsillectomy
I am currently reading John Wennbergs "Tracking Medicine". There are some great insights, and I cannot recommend it enough. One of the most striking pieces I came across relates to the belief, now vanished, that tonsillectomy was critical for a healthy childhood:
"The American Child Health Association’s research design used a random sampling of 1,000 New York City school children. On examination by a school physician, 60% were found to have already had a tonsillectomy, and of the remaining 40%, nearly half were deemed in need of the operation. To make sure that no one in need of a tonsillectomy was left out, the association arranged for the children not selected for tonsillectomy to be reexamined by another group of physicians. The second wave of physicians recommended that 40% of these children have the operation. Still not content that unmet need had been adequately detected, the association arranged for a third examination of the twice-rejected children by another group of physicians. On the third try, the physicians produced recommendations that another 44% should have the operation. By the end of the three-examination process, only 65 children of the original 1,000 emerged from the screening examination without a recommendation for tonsillectomy. If the association had put those 65 children through additional rounds of examination, it seems likely that virtually every last one would have been recommended for surgery, a thought that gives new meaning to the phrase “no child left behind.”While we may laugh at such a practice, are we really that different? Look at the variation you practice yourself, let alone the variation amongst your colleagues, and then remember that the variation within an institution is far less than variation between hospitals. As Wennberg says,
"Thus regions have characteristic “surgical signatures” and regions with high rates of a surgery in the early 1990s still tend to have high rates today, and the cumulative effect is to expose large numbers of patients to surgical interventions that they may or may not have wanted."
To screen or not to screen? That is the question.
Screening arouses great passion, well greatish. Sticking to prostate cancer, there has been a back and forth argument for many years. There is no doubt that using prostate specific antigen testing detects many cancers; however the key question remains whether finding these cancers impacts survival. In other words, would many of these men die with rather than because of their prostate cancer. According to Wennberg, if 1000 men are screened for 10 years, 1 cancer will be found and treated successfully, 4 men will die of their cancer regardless and 50 men will be over-diagnosed and over-treated.
A study just published finds that over a 20 year period, there is no differnece in death rate form prostate cancer between those screened and unscreended.
Again, this points to the potential for reducing variation and reducing costs in healthcare.
A study just published finds that over a 20 year period, there is no differnece in death rate form prostate cancer between those screened and unscreended.
Again, this points to the potential for reducing variation and reducing costs in healthcare.
Simulation
There is increasing interest in the benefits of simulation to ensure improved outcomes in healthcare. A piece in the Economist piqued my interest in this area. They describe a story I had never heard before, involving the role of former US President Jimmy Carter in dealing with a reactor meltdown in Canada in 1952. Carter led a 23 man team to disassemble a reactor near Ottawa that partially melted down. Such was the radiation exposure that each person was limited to 90 seconds at the core. To ensure that the process went as smoothly as possible in such adverse conditions,
"The team built an exact replica of the reactor on a nearby tennis court, and had cameras monitor the actual damage in the reactor's core. "When it was our time to work, a team of three of us practised several times on the mock-up, to be sure we had the correct tools and knew exactly how to use them. Finally, outfitted with white protective clothes, we descended into the reactor and worked frantically for our allotted time," he wrote. "Each time our men managed to remove a bolt or fitting from the core, the equivalent piece was removed on the mock-up."The take home message is no surprise, simulation to be successful must be as realistic as possible, with real time feedback. A paper published in January in PCCM reports that with increasing use of simulation of cardiac arrest in a children's hospital, survival post cardiac arrest increased to 50%, substantially above the national average.
Saturday, April 2, 2011
Bertrand Russell on the scientific method
"Aristotle maintained that women have fewer teeth than men; although he was twice married, it never occurred to him to verify this statement by examining his wives' mouths"
Friday, April 1, 2011
Dr Yoda & the Pirates of the Caribbean
Rather than review some health related news stories, I thought Dr ZDogg would do a better job.
Have a great weekend.
Have a great weekend.
Angry Bird Medicine
A wonderful title to a great blog entry on the BMJ blogs site. Talking about reducing medicine to an App that can be downloaded to ones phone. He has a fantastic quote, “6 years of medical school and 10 years of training can now be put onto an App and sold for a few dollars – where did I go wrong?”
I dont think a 99 cent app on your phone is going to take the place of a doctor just yet, but the natural progression is that knowledge becomes a commodity, it moves down the value chain, and it no longer becomes cost effective for a particular expert to broker that knowledge. So for example, there is no reason why someone with hypertension cant be monitored at home, blood pressure readings relayed by phone to a central station and feedback given around diet, medications etc, all without the person ever leaving home.
I dont think a 99 cent app on your phone is going to take the place of a doctor just yet, but the natural progression is that knowledge becomes a commodity, it moves down the value chain, and it no longer becomes cost effective for a particular expert to broker that knowledge. So for example, there is no reason why someone with hypertension cant be monitored at home, blood pressure readings relayed by phone to a central station and feedback given around diet, medications etc, all without the person ever leaving home.
Disruptive Innovation & healthcare education
One of the great difficulties in bringing safety and quality to the fore in healthcare is that although it impacts everyone, no specialty sees it as their responsibility to take the lead, itself a damning sign of the inability of the profession to see the critical merits of teamwork and systems thinking. The IHI set up its Open School some years ago in an attempt to bring this knowledge directly to healthcare students. My impression is that it is certainly proving successful, but it is the nature of such developments to take many years to fully bear fruit. But bear fruit it will. The message is too compelling and students will naturally ask why they are not being exposed to this area by their own teachers. It's all part of a bottom up approach to change. As an example, I suggest you check out this video, part of the course materials for the Open School.
Learned Helplessness
It has struck me repeatedly that there is a huge degree of learned helplessness in the public sector around the world. I am unsre why this should be the case. Does it reflect a risk averse culture? An overly bureaucratic one in which every action must be backed by a memo? Who knows? The great pity is that one of the great motivating forces for skilled professionals is to have pride and autonomy on their work. See the video, (thanks John F) for a great example of the phenomenon.
Public Reporting of Surgical Outcomes
In this weeks Lancet, a discussion around public reporting of surgical outcomes. Specific mention is made of the Society for Cardiothoracic Surgery in Great Britain and Ireland. Since 2005, the society has made outcome data freely available to the public; this has been associated with a 50% reduction in risk adjusted mortality, i.e. half as many people have died as would have been expected to die.
In terms of cost savings, the program costs £1.5 million annually, but is estimated to save £5 million per year in reduced length of stay costs.
In terms of cost savings, the program costs £1.5 million annually, but is estimated to save £5 million per year in reduced length of stay costs.
While clinicians may be resistant to public reporting of data, it is inevitable. My opinion is that it is better to be proactive, seek to develop such databases and ensure the data represents as accurately as possible the reality, i.e. risk adjusted.
Trends in youth mortality around the world
Published in The Lancet today, an analysis of WHO data looking at mortality trends in children and young adults around the world over the last 50 years. There have been dramatic improvements in mortality reduction around the world, as much as a 93% reduction in children aged 1-4. The smallest reduction occurred in young men, aged 15-24. More focus should be directed on reducing mortality in this group. However, this is a very encouraging and optimistic paper, showing that greta work can be achieved.
Statistics for dummies.
For anyone who love data, check this out. Rosling is magnificent and can summarise in 4 minutes of pictures what may are unable to do in a book. Wealth increases health.
Also see his website. www.gapminder.org
Also see his website. www.gapminder.org
Reduced work hours for doctors
In both Europe and the US, there has been a push to reduce the hours worked by doctors. This has been based on the belief that tired doctors make more mistakes. An article in this weeks BMJ points out that to date there is no evidence that these measures have brought about an improvement in safety. Why should this be? There are many possible explanations, but in my view, these reductions in working hours have been implemented without taking a fundamental look at how doctors work. in other words, a dramatic change in work hours should have been accompanied by a radical restructuring of shifts, handovers, continuity and so on. It is likely that this has not occured. The other problem is that junior doctors work hour and patterns evolved to match those of senior physicians. The work patterns of these senior doctors also needs to be considered and modified.
Thank you for the music
Falls are an major problem for the elderly. An interesting piece in this weeks Archives of Internal Medicine reports that using music to in effect co-ordinate walking substantially reduces the risk of falls in a community based elderly population.
Thursday, March 31, 2011
How to wash your hands properly in hospital
Great video from NEJM, free to view. Obligatory for all healthcare staff, (and also patients, families, kids so they can be sure their carers are doing it the right way.)
Immunisation
I was going to do a piece on immunization. These guys do a far better job than I ever could. Check out zdoggmd.com
Wednesday, March 30, 2011

Overdiagnosis
A fantastic piece in the Archives of Internal Medicine, about incidental findings (incidentalomas) picked up while testing for something else. This opens up a whole Pandoras box. A great line about a New York Times columnist who believed he had survived a brush with death following the finding of one such incidentaloma. No, the authors say, he survived a brush with overdiagnosis.
This is very important. The fundamental issue is that each patient will feel they have been saved and each becomes an advocate for more and more testing. However, there is no evidence that many of these findings, even if malignant, will ever pose a threat to health. The authors provide some practical suggestions as to how best to approach these matters.
This is very important. The fundamental issue is that each patient will feel they have been saved and each becomes an advocate for more and more testing. However, there is no evidence that many of these findings, even if malignant, will ever pose a threat to health. The authors provide some practical suggestions as to how best to approach these matters.
Clinically Integrated Systems
Following on from my thoughts about disruptive innovation, what structures in the UK and Irish setting might prove disruptive? Starting from the assumption, which may be mistaken, that some disruptors will be players in the current system, what could one possible future look like?
I believe the likeliest candidates are current general practice and primary care structures. They have the benefit of decent infrastructure, a critical mass of clinical, (not just medical) staff, and a population base that is large and varied enough to allow sub-specialistation. What are the missing ingredients?
I believe the likeliest candidates are current general practice and primary care structures. They have the benefit of decent infrastructure, a critical mass of clinical, (not just medical) staff, and a population base that is large and varied enough to allow sub-specialistation. What are the missing ingredients?
- Seamless integration between priamry care and hospitals; to deliver this, I believe there needs to be consultant presence in the primary care teams. Consultants would work between hospital and primary care, with benefits to staff and patients, (improved access to specialist opinion, greater communication between professionals, enhanced learning opportunities for all)
- A payment system that rewards health, and is not just based on following processes, (e.g. check blood pressure every visit). What would this look like? Look at it from the patient perspective. What he/she wants is health, as few visits as possible, as little interruption to daily life, mot missing school or work. Can this be done. I believe it can, but it will require a fundamental shift in the way health, (as opposed to healthcare) is delivered.
- A recognition that an unplanned hospital admission represents a failure of care for the team providing care
- Quality and outcome metrics allied with an IT system sensitive enough to provide real time data
There is an interesting paper just published on the BMJ site by Chris Ham discussing this. They report the experience of Torbay, summarised below:
- Reduced use of hospital beds (daily average number of occupied beds fell from 750 in 1998-9 to 502 in 2009-10)
- Low use of emergency bed days among people aged ≥65 (1920/1000 population compared with regional average of 2698/1000 population in 2009-10)
- Minimal delayed transfers of care
"hospital providers could also take the initiative in moving in this direction, especially in areas where general practitioners are relatively weak and specialists strong. London is a case in point, not least because it has several academic health sciences centres that present the potential to extend high quality care from hospitals into the community. In this context, integration might build on the strengths of academic health sciences centres by allocating them a capitated budget in conjunction with general practitioners and community health service providers. Patients would be able to choose between integrated systems based on academic health sciences centres and could also access care outside these systems in order to create an incentive for providers to deliver responsive care of high quality."
Are guidelines tainted?
One of the truisms of healthcare is that we should adhere to guidelines in so far as possible, to reduce variation, to improve outcomes and to minimize waste. Guidelines are developed by eminent professionals in a field; it is assumed that they are guided only by the evidence. However, many of these guidelines are sponsored by pharma companies.
A study just published in the Archives of Internal Medicine examined conflicts of interest amongst panel members charged with developing almost 20 cardiology guidelines. They find that 56% of panel members have a declared conflict of interest, e.g. owning stock in a company whose product is recommended, and 81% of panel leaders have a COI. That is not to say that these were unduly influenced by these conflicts, but some wonder whether like Caesars' wife, all should be above suspicion.
One suggestion is to prohibit all guideline developers to have a COI; my own view on this is that it may just exclude those who have the most to offer.
A study just published in the Archives of Internal Medicine examined conflicts of interest amongst panel members charged with developing almost 20 cardiology guidelines. They find that 56% of panel members have a declared conflict of interest, e.g. owning stock in a company whose product is recommended, and 81% of panel leaders have a COI. That is not to say that these were unduly influenced by these conflicts, but some wonder whether like Caesars' wife, all should be above suspicion.
One suggestion is to prohibit all guideline developers to have a COI; my own view on this is that it may just exclude those who have the most to offer.
How the iPhone is going to save the world. Seriously!
An artist with an interest in healthcare recently asked me for my thoughts about the future direction of art (broadly defined) in children's healthcare. It's not an area to which I had given much thought but it caused me to consider the benefits, if any, of art and media in healthcare. Simply put, how best to use that which is the favorite activity of children, playing, to assist them in the treatment of their illness.
Just published in JAMA yesterday is a commentary which outlines some of the potential uses and benefits of video games. Before anyone rubbishes the concept, there are good precedents here. My younger patients undergoing a lung function test in which they must breathe into a machine as fast as possible are encouraged to do so by a screen with a birthday cake and candles; the harder they blow, the more candles are extinguished.
The paper in JAMA describes various tools. Mindless Eating Challenge, a weight loss program, is a game where users support one another by sharing photographs of portion sizes. Lit to Quit allows iPhone users to puff into the phone to simulate the experience of smoking.
While the skeptics may rightly laugh off these efforts, bear in mind these are very early days. Analogous to measuring urine glucose in diabetics in the 1920's. This took 5 minutes using some very sophisticated reagents. Underestimate the power of technology at your peril.
While I am not an expert in this area, it seems to me that the real focus of opportunity lies in the nexus of massive multiplayer on line games (MMOG) and social networking. Christakis has published a number of very significant papers showing the effects of social networks on depression, happiness, weight gain and smoking. Imagine a game, aimed at children with diabetes, where children can interact and earn from one another, in which the game incentivizes the appropriate behaviors, such as diet, exercise, compliance with screening and so on. Crazy? Yes, without a doubt. Crazier than our current system where we believe that seeing a child a few times a year in a busy environment with numerous distractions is going to deliver the best outcomes? You decide.
Just published in JAMA yesterday is a commentary which outlines some of the potential uses and benefits of video games. Before anyone rubbishes the concept, there are good precedents here. My younger patients undergoing a lung function test in which they must breathe into a machine as fast as possible are encouraged to do so by a screen with a birthday cake and candles; the harder they blow, the more candles are extinguished.
The paper in JAMA describes various tools. Mindless Eating Challenge, a weight loss program, is a game where users support one another by sharing photographs of portion sizes. Lit to Quit allows iPhone users to puff into the phone to simulate the experience of smoking.
While the skeptics may rightly laugh off these efforts, bear in mind these are very early days. Analogous to measuring urine glucose in diabetics in the 1920's. This took 5 minutes using some very sophisticated reagents. Underestimate the power of technology at your peril.
While I am not an expert in this area, it seems to me that the real focus of opportunity lies in the nexus of massive multiplayer on line games (MMOG) and social networking. Christakis has published a number of very significant papers showing the effects of social networks on depression, happiness, weight gain and smoking. Imagine a game, aimed at children with diabetes, where children can interact and earn from one another, in which the game incentivizes the appropriate behaviors, such as diet, exercise, compliance with screening and so on. Crazy? Yes, without a doubt. Crazier than our current system where we believe that seeing a child a few times a year in a busy environment with numerous distractions is going to deliver the best outcomes? You decide.
Tuesday, March 29, 2011
Healthcare; time to be disrupted.
A disruptive innovation (the term was first coined by Clay Christensen) is a technology or strategy, which disrupts an existing market by radically lowering price, increasing productivity or by gaining an alternative set of customers. Examples include the transition from sail to steamships, the adoption of personal computers in place of mainframes and so on. Henry Ford put it well; “to build a better motorcar one could either develop a faster and stronger horse or do something completely different.”
The question for healthcare is whether disruptive innovations are required to radically improve value and outcomes? Alternatively can tinkering with the system, (QIPP, ACO, Medical Homes, pay for performance, increase measurement and accountability) drive sufficient performance and improvement. To truly understand the significance of this question, one has to understand both the power of disruptive innovation and the failure of those agencies being disrupted to challenge the disruption.
Disruptive innovations essentially create a market for a product or service that the incumbents fail to recognize. They do so, often by offering a cheaper, slimmed down product; think Ryanair. One may not like them but they not only offer a cheaper reliable service, but developed a market for services that no-one could have imagined, (London Lodz anyone?).
Existing airlines had no incentive to develop such innovations; they were happy with their quasi-monopolies. Ryanair had to develop such markets in order to grow. if existing companies were to chase these market opportunities, they would cut into their existing markets and reduce their profit margins. In a sense they are helpless to do anything, apart from resisting and fighting back, (think lobbyists, negative advertising campaigns)
Jump to healthcare, the structures are identical. Seemingly strong vested interests, institutional, professional, academic, who will do their best to fight any interloper promising a better cheaper service. And they are helped immensely by the emotional arguments that if the service they offer is undercut, people will die.
Are there examples of such disruption in health? They are likely to appear when the current model no longer makes financial sense, or where Western models are not applicable. It is likely that if this economic downturn persists that we will begin to see disruptors emerge in both the West, and emerge from the developing world into the West. For example, “Aravind the world’s biggest eye-hospital chain, performs some 200,000 eye operations a year. It takes the assembly-line principle literally: four operating tables are laid side by side and two doctors operate on adjacent tables. When the first operation is done, the second patient is already in place.” (Economist April 2010)
A paper by Robert Brook of the RAND corporation outlined one vision of potential disruptors. These include:
The question for healthcare is whether disruptive innovations are required to radically improve value and outcomes? Alternatively can tinkering with the system, (QIPP, ACO, Medical Homes, pay for performance, increase measurement and accountability) drive sufficient performance and improvement. To truly understand the significance of this question, one has to understand both the power of disruptive innovation and the failure of those agencies being disrupted to challenge the disruption.
Disruptive innovations essentially create a market for a product or service that the incumbents fail to recognize. They do so, often by offering a cheaper, slimmed down product; think Ryanair. One may not like them but they not only offer a cheaper reliable service, but developed a market for services that no-one could have imagined, (London Lodz anyone?).
Existing airlines had no incentive to develop such innovations; they were happy with their quasi-monopolies. Ryanair had to develop such markets in order to grow. if existing companies were to chase these market opportunities, they would cut into their existing markets and reduce their profit margins. In a sense they are helpless to do anything, apart from resisting and fighting back, (think lobbyists, negative advertising campaigns)
Jump to healthcare, the structures are identical. Seemingly strong vested interests, institutional, professional, academic, who will do their best to fight any interloper promising a better cheaper service. And they are helped immensely by the emotional arguments that if the service they offer is undercut, people will die.
Are there examples of such disruption in health? They are likely to appear when the current model no longer makes financial sense, or where Western models are not applicable. It is likely that if this economic downturn persists that we will begin to see disruptors emerge in both the West, and emerge from the developing world into the West. For example, “Aravind the world’s biggest eye-hospital chain, performs some 200,000 eye operations a year. It takes the assembly-line principle literally: four operating tables are laid side by side and two doctors operate on adjacent tables. When the first operation is done, the second patient is already in place.” (Economist April 2010)
A paper by Robert Brook of the RAND corporation outlined one vision of potential disruptors. These include:
- Considering the entire cost of care, to include not just the cost to the individual but the energy cost, (carbon cost)
- Unifying the two great silos of medicine and education so that educators play a central role in improving children’s health and healthcare providers are judged partly on their success at improving educational attainment in their patients
- A shift to non-physican care, e.g. nurse practitioners
- Reduce the training required for repetitive technical task; for example why go to medical school, residency and fellowship to train how to remove cataracts. Pretty radical.
- Routine healthcare delivered 24/7. So no more 9-5 operating rooms or clinics.
- Outsourcing or off-shoring of many tasks, including diagnostics, elective surgery which is already happening.
Innovation
For some reason, posting a lot of stuff from the WSJ recently, but it's all good. Check out this piece about the need to innovate in healthcare.
"Unlike many other industries, health care has remained highly fragmented, with a hierarchical culture resistant to change, and a payment system that rewards providers for quantity rather than quality of care. It has been slow to adopt technologies like electronic medical records that have the potential to make care more efficient and safer for patients. Even when new practices have been shown to improve care and reduce error, hospitals and doctors have been slow to adopt them."
"Unlike many other industries, health care has remained highly fragmented, with a hierarchical culture resistant to change, and a payment system that rewards providers for quantity rather than quality of care. It has been slow to adopt technologies like electronic medical records that have the potential to make care more efficient and safer for patients. Even when new practices have been shown to improve care and reduce error, hospitals and doctors have been slow to adopt them."
Pronovost
Great piece in todays Wall Street Journal, an interview with Pronovost, well worth reading.
Monday, March 28, 2011
Europe's Failing Health (Systems)
Great piece in todays Wall Street Journal. Discusses the challenges facing healthcare systems, from the funding perspective, throughout Europe. My favourite line,
"In 1995 the cost of a hip replacement was the equivalent of buying a flat-screen TV in Germany," he says. "In 2008 you could get 10 flat-screen TVs for the amount of money you paid for a hip replacement."
"In 1995 the cost of a hip replacement was the equivalent of buying a flat-screen TV in Germany," he says. "In 2008 you could get 10 flat-screen TVs for the amount of money you paid for a hip replacement."
The conclusion? Healthcare funding and design must change, and change radically.
Does improving quality save money?
The instinctive answer is, "yes, of course." If only it were that easy. I am more and more coming around to the view that to change a complex system like healthcare will require radical restructuring, which will only happen in the Western World when we realise we can no longer afford to deliver our current service. It wont be easy, it wont be pleasant.
Levette has sent me a paper which suggests that improved quality and lower costs may not go hand in hand. Bottom line;
"The evidence suggests that there are ways of saving money at the same time as improving quality. But doing so on a large scale requires changes in how services are financed, and increasing the capability of ordinary services to make changes. Approaches that look effective in theory rarely seem to have the same impact when implemented in practice and on a large scale. In this respect, the challenges of achieving real finan- cial savings by improving quality and reducing waste are no different from any other attempt to change a complex system."
Levette has sent me a paper which suggests that improved quality and lower costs may not go hand in hand. Bottom line;
"The evidence suggests that there are ways of saving money at the same time as improving quality. But doing so on a large scale requires changes in how services are financed, and increasing the capability of ordinary services to make changes. Approaches that look effective in theory rarely seem to have the same impact when implemented in practice and on a large scale. In this respect, the challenges of achieving real finan- cial savings by improving quality and reducing waste are no different from any other attempt to change a complex system."
Training for the future: from 20th century medicine to 21st century healthcare delivery
Check out this great piece from Peter Lachman. Nicely aligns with what I wrote about yesterday.
Disruptive Innovation
Hope to write a bit today about disruptive innovation in healthcare. Just to get into the mood. Thanks Lils.
From Apple Computers Think Different (R) campaign.
"Here’s to the crazy ones. The misfits. The rebels. The troublemakers. The round pegs in the square holes. The ones who see things differently. They’re not fond of rules. And they have no respect for the status quo. You can quote them, disagree with them, glorify or vilify them. About the only thing you can’t do is ignore them. Because they change things. They push the human race forward. And while some may see them as the crazy ones, we see genius. Because the people who are crazy enough to think they can change the world, are the ones who do."
From Apple Computers Think Different (R) campaign.
"Here’s to the crazy ones. The misfits. The rebels. The troublemakers. The round pegs in the square holes. The ones who see things differently. They’re not fond of rules. And they have no respect for the status quo. You can quote them, disagree with them, glorify or vilify them. About the only thing you can’t do is ignore them. Because they change things. They push the human race forward. And while some may see them as the crazy ones, we see genius. Because the people who are crazy enough to think they can change the world, are the ones who do."
Sunday, March 27, 2011
Medical Education; Fit for the 21st Century?
My personal view is that the current model of medical education is no longer fit for purpose; it is too heavily oriented to rote learning, is excessively hospital focused, pays little attention to the overwhelming needs of disease prevention, is excessively focused on providing healthcare as opposed to health, does not have a word to say about systems thinking and pays lip service to the concept of teamwork. There is no emphasis on the need to provide value, it does not provide the tools that allow professionals to continuously improve their service and has nothing to say about the economics of health and importantly our obligations as professionals to ensure money is spent to ensure that society receives the maximal benefit.
A very clever intern spoke to me recently, and I was discussing the concept of safety and quality. She told me she had never heard anyone in 6 years of medical school discuss these concepts. A shocking state of affairs.
Which brings me to the purpose of this post. A paper was recently published in the Lancet, and I will let the authors speak for themselves. Fundamentally, it is a call to arms, laying out the clear need to radically reform the model of medical education, in similar fashion to the Flexner report 100 years.
"Professional education has not kept pace with these challenges, largely because of fragmented, outdated, and static curricula that produce ill-equipped graduates. The problems are systemic: mismatch of competencies to patient and population needs; poor teamwork; persistent gender stratification of professional status; narrow technical focus without broader contextual understanding; episodic encounters rather than continuous care; predominant hospital orientation at the expense of primary care; quantitative and qualitative imbalances in the professional labour market; and weak leadership to improve health-system performance. Laudable efforts to address these deficiencies have mostly floundered, partly because of the so-called tribalism of the professions—ie, the tendency of the various professions to act in isolation from or even in competition with each other.
Redesign of professional health education is necessary and timely, in view of the opportunities for mutual learning and joint solutions offered by global interdependence due to acceleration of flows of knowledge, technologies, and financing across borders, and the migration of both professionals and patients. What is clearly needed is a thorough and authoritative re-examination of health professional education, matching the ambitious work of a century ago."
A very clever intern spoke to me recently, and I was discussing the concept of safety and quality. She told me she had never heard anyone in 6 years of medical school discuss these concepts. A shocking state of affairs.
Which brings me to the purpose of this post. A paper was recently published in the Lancet, and I will let the authors speak for themselves. Fundamentally, it is a call to arms, laying out the clear need to radically reform the model of medical education, in similar fashion to the Flexner report 100 years.
"Professional education has not kept pace with these challenges, largely because of fragmented, outdated, and static curricula that produce ill-equipped graduates. The problems are systemic: mismatch of competencies to patient and population needs; poor teamwork; persistent gender stratification of professional status; narrow technical focus without broader contextual understanding; episodic encounters rather than continuous care; predominant hospital orientation at the expense of primary care; quantitative and qualitative imbalances in the professional labour market; and weak leadership to improve health-system performance. Laudable efforts to address these deficiencies have mostly floundered, partly because of the so-called tribalism of the professions—ie, the tendency of the various professions to act in isolation from or even in competition with each other.
Redesign of professional health education is necessary and timely, in view of the opportunities for mutual learning and joint solutions offered by global interdependence due to acceleration of flows of knowledge, technologies, and financing across borders, and the migration of both professionals and patients. What is clearly needed is a thorough and authoritative re-examination of health professional education, matching the ambitious work of a century ago."
The Great Crack Up
"The test of a first-rate intelligence is the ability to hold two opposed ideas in the mind at the same time, and still retain the ability to function. One should, for example, be able to see that things are hopeless and yet be determined to make them otherwise."
F.Scott Fitzgerald, The Great Crack-up, 1936
I think the quote above will resonate with many of those who faced with the daily challenge of improving a health service still believe it is possible.
F.Scott Fitzgerald, The Great Crack-up, 1936
I think the quote above will resonate with many of those who faced with the daily challenge of improving a health service still believe it is possible.
Is informed consent bad for your health?
A letter in this weeks Lancet is worth considering. Having been involved in a number of clinical studies in paediatric intensive care units, this resonated with me. The purpose of seeking informed consent from an individual enrolled in a clinical study is to ensure that they are protected in so far as possible and are fully aware of any possible risks entering this study may entail. The benefits of enrolling in a study, apart from the societal good of increasing knowledge is that there is some evidence that patients in a clinical study, regardless of whether they receive the experimental treatment or conventional treatment receive better quality of care. There is also the possibility that they may benefit from the experimental intervention.
Using data from the CRASH trial, researchers estimated that in hospitals which sought consent from relatives, there was a 1.2 hour delay in initiating treatment compared to those hospitals in which no consent was sought. Applying these data to an analysis of the CRASH-2 trial, the researchers estimated that a one hour delay in commencing treatment resulted in a reduction in the percentage of patients responding to treatment from 63% to 49% with a likely increase in death and disability being the result.
There are two consequences; first the delay results in an increased risk of poor outcomes, second, the delay may obscure benefits that accrue from administering a time sensitive treatment.
This has important ethical and scientific implications.
Using data from the CRASH trial, researchers estimated that in hospitals which sought consent from relatives, there was a 1.2 hour delay in initiating treatment compared to those hospitals in which no consent was sought. Applying these data to an analysis of the CRASH-2 trial, the researchers estimated that a one hour delay in commencing treatment resulted in a reduction in the percentage of patients responding to treatment from 63% to 49% with a likely increase in death and disability being the result.
There are two consequences; first the delay results in an increased risk of poor outcomes, second, the delay may obscure benefits that accrue from administering a time sensitive treatment.
This has important ethical and scientific implications.
Saturday, March 26, 2011

Are you better off flying with a trainee pilot, or being operated on by a trainee surgeon?
One of the concerns that some people have relates to the way we train our doctors, essentially an apprenticeship system, with a trainee learning from a senior doctor. While I have some concerns about other aspects of this system, one of the unavoidable consequences is that trainees have to practice upon a patient. Is this safe? Surely being operated on by someone with less expertise increases the risk of something going wrong?
A study has just been published seeking to answer that question. The American College of Surgeons examined patient outcomes in more than 600,000 operations. They found that having a resident, (junior surgeon in training) while associated with a slightly higher risk of developing (usually minor) complications, was also more likely to be associated with a slightly reduced risk of death. The reasons obviously are unclear, but this important paper does provide some reassurance.
A study has just been published seeking to answer that question. The American College of Surgeons examined patient outcomes in more than 600,000 operations. They found that having a resident, (junior surgeon in training) while associated with a slightly higher risk of developing (usually minor) complications, was also more likely to be associated with a slightly reduced risk of death. The reasons obviously are unclear, but this important paper does provide some reassurance.
Wow, Oh Wow
That was Muir Grays Twitter post on seeing this weeks BMJ. Apart from the papers referenced below (Reducing Variation March 24th), there are a number of other papers worth checking out. A report from the Netherlands again finds a marked variation in utilization of medical interventions. An editorial on variation in the NHS; a look at how to redevelop care for long term conditions, and a lot more.
Why such emphasis on variation? Surely the areas with low utilization will balance out the high users for a zero sum game. This is unlikely to be the case, there is mounting evidence, mainly from the US, but also from other countries, that outcomes are not affected by the amount of care given above a certain amount. Therefore there are huge opportunities for reducing waste, saving money, and a lot more good stuff.
Why such emphasis on variation? Surely the areas with low utilization will balance out the high users for a zero sum game. This is unlikely to be the case, there is mounting evidence, mainly from the US, but also from other countries, that outcomes are not affected by the amount of care given above a certain amount. Therefore there are huge opportunities for reducing waste, saving money, and a lot more good stuff.
Thursday, March 24, 2011

Eliminate Variation, Part 2
A piece in the BMJ by John Wennberg summarizes much of the knowledge around variation in medical practice. He breaks unwanted variation into three categories, effective care, preference sensitive care and supply sensitive care.
- Effective care. This is care that is the right treatment for the vast majority of patients, and variation in this element relates to underuse, e.g. vaccination
- Preference Sensitive Care. This is care provided when there are more than one effective treatment, and choice of therapy should be dictated by patient preference; in fact, physician choice often determines this. Mastectomy rather than lumpectomy plus radiation for breast cancer for example.
- Supply sensitive care. This is care that is dependent on the supply of services in a region. Roehmers law is one example of this; this states that in an insured popualtion, a hosoital bed is a filled bed. Dartmouth have found no corrleation between the amount of care received and outcomes, suggesting that there are areas with massive overuse of resources. Gawande in a brilliant article two years ago examined this discrepancy.
Also check out the NHS health Atlas. There are huge variations in care evident. Likely that this occurs everywhere.
Eliminate Variation
One of the godfathers of determining the extent of variation in medical practice and founder of the Dartmouth Health Atlas, Jack Wennberg, has recently published a book, "Tracking Medicine", available here. I have just downloaded it, will review it when finished, but it gets a great review here.

Wednesday, March 23, 2011

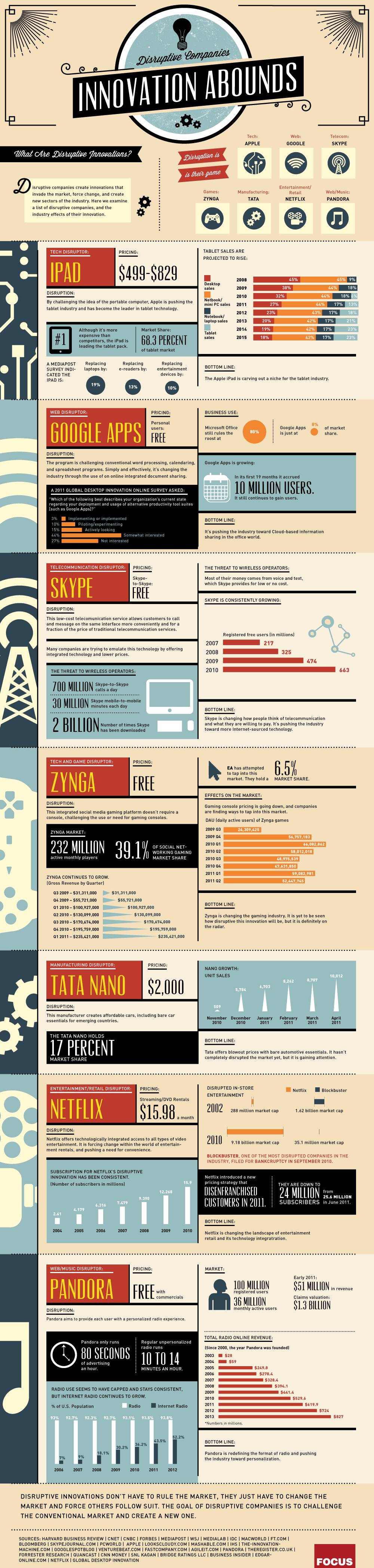{kind=link}
Subscribe to:
Posts (Atom)