
The reasonable man adapts himself to the world; the unreasonable one persists in trying to adapt the world to himself. Therefore, all progress depends on the unreasonable man. GB Shaw
Thursday, November 3, 2011
The system is dead, long live the system
If you believe, as I do, that the current model of Western healthcare delivery is dying, I suggest you read this piece. Medicine is succumbing to the disease that infects all large human endeavors, the current structures seek to justify and build upon themselves. Even if done for the best of reasons, the usual solution sought from heath care workers is to build more of the same, buy more of the same, do more of the same. I see many parallels between the military industrial complex that worried Eisenhower, and our current medical industrial complex.
Tuesday, October 18, 2011
Escape Fire and high reliability
I have bene rereading two books recently, Managing the Unexpected, (a fantastic read) and Berwicks Escape Fire. Berwick spoke about the Mann gulch fire disaster in Montana, about which Weick has written. Although at first pass, one wonders what lessons a forest fire in Montana has to delivering safe care in health, there are many deep lessons to be learned. This is a paper well worth reading. A few examples.
Partners and partnership are critical.
To be wise is not to know particular facts but to know without excessive confidence or excessive cautiousness. Wisdom is thus not a belief, a value, a set of facts, a corpus of knowledge or information in some specialized area, or a set of special abilities or skills. Wisdom is an attitude taken by persons toward the beliefs, values, knowledge, information, abilities, and skills that are held, a tendency to doubt that these are necessarily true or valid and to doubt that they are an exhaustive set of those things that could be known.
In a fluid world, wise people know that they don't fully understand what is happening right now, because they have never seen precisely this event before. Extreme confidence and extreme caution both can destroy what organizations most need in changing times, namely, curiosity, openness, and complex sensing. The overconfident shun curiosity because they feel they know most of what there is to know. The overcautious shun curiosity for fear it will only deepen their uncertainties. Both the cautious and the confident are closed-minded, which means neither makes good judgments. It is this sense in which wisdom, which avoids extremes, improves adaptability.
Partners and partnership are critical.
A partner makes social construction easier. A partner is a second source of ideas. A partner strengthens independent judgment in the face of a majority. And a partner enlarges the pool of data that are considered. Partnerships that endure are likely to be those that adhere to Campbell's three imperatives for social life, based on a reanalysis of Asch's (1952) conformity experiment:
(1) Respect the reports of others and be willing to base beliefs and actions on them (trust);
(2) Report honestly so that others may use your observations in coming to valid beliefs (honesty); and,
(3) Respect your own perceptions and beliefs and seek to integrate them with the reports of others without deprecating them or yourselves (self-respect).
Wednesday, October 12, 2011
Motivation and work satisfaction.
Reading Quality by Design; well worth delving into. A quote by Paul O'Neill, ex CEO of Alcoa and Former Secretary of the US Treasury.
"I am treated with dignity and respect everyday by everyone i encounter... and it doesn't have anything to do with hierarchy. I'm given the opportunity and the tools that i need to make a contribution and this gives meaning to my life. Someone noticed that I did it.O'Neill states that a high level of work-life satisfaction exists when every employee can strongly agree with these three statements. A simple approach, too often disregarded in health organisations.
Monday, October 10, 2011
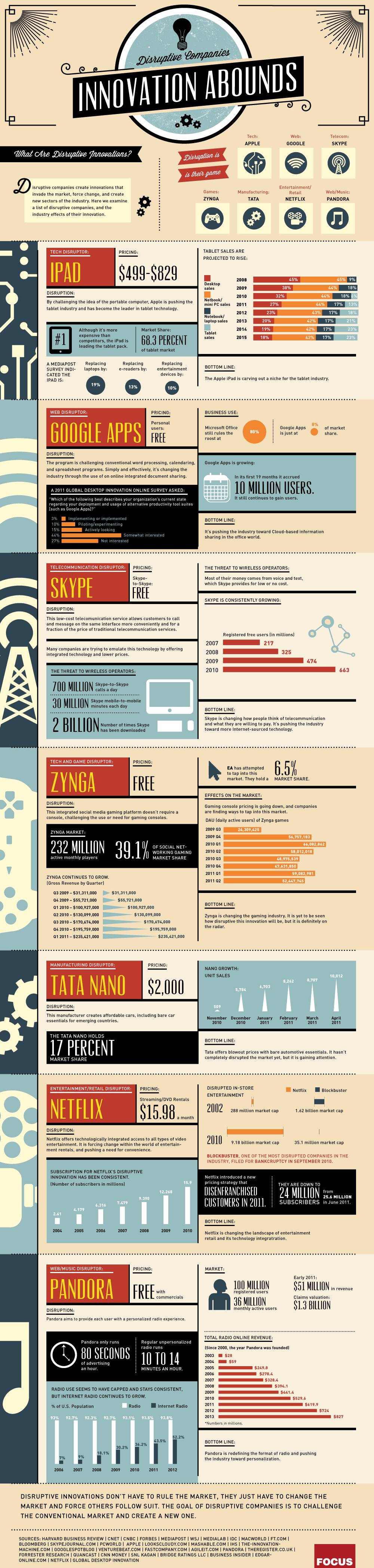
Disruptive Innovation
From one of my fave blogs, The Big Picture, comes a great graphic about disruptive innovation. Bottom line;
Disruptive innovations don't have to rule the market, they just have to change the market and force others to follow suit. The goal of disruptive companies is to challenge the conventional market and create a new one.
Monday, October 3, 2011
Improve patient experience and staff experience
I read a few days ago two articles in BMJ Quality and Safety, (here and here, sorry sub required) in which patients recounted their experiences, (pretty bad). A letter in response makes the point that addressing the defects that result in poor care not only improves the patient experience, but also makes work more satisfying for staff. A true win-win.
"Frontline staff frequently struggle with infrastructure issues that inhibit their ability to deliver high quality care, undermine their work flow and also affect their morale. Many of these same infrastructure problems frustrate patients as much as they do staff. Some patient safety problems thus represent a win–win situation from an organisation's point of view: addressing them improves patient safety and increases the efficiency of frontline staff, as well as the quality of their work life."
Safety in Primary Care
Safety in hospital care (or the lack of) gets the lions share of attention. However, little is known about safety in primary care; even if substantially safer, there may still be substantial risks given the huge numbers who access care through their GP as compared to the numbers accessing hospital services. A piece that discussed this subject is published here by BMJ.
"Do we really know how safe general practice is? And where we identify problems, what sort of mechanisms do we have to ensure that the sort of poor practice that the programme identified is addressed? "
Sunday, October 2, 2011
ZDOGG
I must admit, I love ZDOGG MD. This piece is a classic. Mental Illness on Sesame Street. Check it out, it will cheer your day.
Whistleblowing
I hate the term "whistleblower". It has all sorts of negative connotations, for doing something that is intended to stop bad behaviour, bad practice, and harm. At a meeting in London two years ago, i heard 3 "whistleblowers", all non-medical talk about their experience. they found it very harrowing, and i seem to recall all three saying they would never do it again. See here for a link to one of the speakers. Just a few days ago, I came across this piece, the story of the anesthetist who raised concerns about poor outcomes in children and babies undergoing heart surgery in Bristol.
A damning indictment.
Leaving the UK with my wife and family was an incredibly sad and disappointing time but I am sure now that there could never have been ‘Clinical Governance’ or a change in medical attitudes while I remained in the UK. Only when I had a contract in a new hospital, in a new country did I feel secure enough to report the mortality rate in the Bristol paediatric cardiac surgery unit to the GMC. Sadly despite the Presidents and Council Members of 2 Royal Colleges, the Dean of the Medical School, numerous Professors, some members of the Trust Board, members of the Department of Health and many local clinicians all knowing about Bristol, no other doctors in the UK reported these events to the GMC. I believe that this is a serious and permanent indictment of the attitudes of the profession that prevailed at that time and persist in some quarters in the UK. At least 12 sets of parents had reported deaths to the GMC, but their complaints would not have been investigated without a complaint from a doctor.
A damning indictment.
Friday, September 30, 2011
Risky Business
A report has just been published by the Royal College of Surgeons of England entitled “The Higher Risk General Surgical Patient: towards improved care for a forgotten group”. It is a very sobering examination of the outcome in non cardiac emergency surgery.
My pet interest of variation in care and outcomes is addressed.
Higher risk non-cardiac general surgery is undertaken in every acute hospital. By way of comparison, the mortality for this group, which includes most major gastro-intestinal and vascular procedures, exceeds that for cardiac surgery by two to three fold and complication rates of 50% are not uncommon. There may be a lack of awareness of the level of risk. Among these patients, emergency surgery and unscheduled management of complications is common and this group of patients are one of the largest consumers of critical care resources. The health and financial costs are considerable.The most amazing statistic in this paper is the fact that “Complications occur in as many as 50% of patients undergoing some common procedures.”
My pet interest of variation in care and outcomes is addressed.
Review of 2008/9 hospital episode statistics (HES) data from Dr Foster reveal a greater than two-fold variation in relative risk of 30-day mortality (risk-adjusted) after non-elective lower GI procedures between trusts in the North West SHA (strategic health authority). It is known that the chance of a patient dying in a UK hospital is 10% higher if he or she is admitted at a weekend rather than during the week.Anyone involved in ensuring good outcomes for surgical patients, or ensuring that hospital resources are used efficiently, (by reducing unnecessary complications) needs to read this.
Thursday, September 29, 2011
Normalisation of Deviance
One of my favourite terms is the “Normalisation of Deviance”. I think it captures perfectly what happens every day in healthcare. We work around problems, pat ourselves on the back for finding a (temporary) solution, and ignore the very profound message that the system is sending us; this message essentially is “you dont understand your system and your processes and if you dont work out a way to fix this problem, there will be serious consequences”. In Reasons Swiss Cheese model, all those little holes are problems that usually were recognised well before a serious event occured, but were most often ignored and certainly never consciously addressed and removed.
As Scott Snook, a lecturer from Harvard puts it:
As Scott Snook, a lecturer from Harvard puts it:
Each uneventful day that passes reinforces a steadily growing false sense of confidence that everything is all right – that I, we, my group must be OK because the way we did things today resulted in no adverse consequences.A paper that describes the consequences of this thinking, really a form of magical thinking is available on the NASA website; it is a section of the report into the Columbia Space Shuttle disaster. Available here.
Deming, why now?
A piece worth reading, published by the Deming Collaboration, and authored by Rafael Agauyo, who studied with Deming and subsequently published a book about Deming and his methods, (which is an excellent overview). Although there is a danger of assuming that one persons hero is the answer to all the worlds problems, Deming has outlined a systematic approach; contrast this with the toolbox approach, i.e. lets introduce lean or TQM or some other method de jour, stand back and watch our performance improve. Although Deming is probably best known for his PDSA, or PDCA cycle, his more profound contribution was the System of Profound Knowledge.
Coaching
A great and as ever thought provoking piece from Gawande. He discussed the value of coaching and describes his experience and initial results of using a surgical coach. Well worth a read.
Wednesday, September 28, 2011
Hard Jobs
A quote attributed to Peter Drucker, one of the great management gurus:
I find that hard to believe, but on mature reflection, maybe not.
- “The four hardest jobs in America (not necessarily in order) are: President of the United States, a university president, a hospital CEO, and a pastor.”
- “Health care is the most difficult, chaotic, and complex industry to manage today.”
- “The hospital is altogether the most complex human organization ever devised.”
Thursday, September 15, 2011
Physician Burnout
Physician burnout is a well recognised problem, and may be associated with other undesirable factors including substance abuse, depression, physician suicide and poor patient outcomes. I am seeing the phenomenon of burnout more frequently, but my impression is that the response of the system is not just to ignore this but to continue to pile on more pressure.
A paper just published here reports some very disturbing findings.
A paper just published here reports some very disturbing findings.
Quality of life was rated “as bad as it can be” or “somewhat bad” by 2402 of 16 187 responding residents (14.8%). Overall burnout and high levels of emotional exhaustion and depersonalization were reported by 8343 of 16 192 (51.5%), 7394 of 16 154 (45.8%), and 4541 of 15 737 (28.9%) responding residents, respectively.Interestingly, international medical graduates showed lower levels of distress. The fundamental problem in my view is that physicians refuse to recognize these problems in their colleagues and indeed see such problems as “weakness and failure”
One factor in the difficulty in ensuring change happens in healthcare is that healthcare workers, especially doctors, find it easy to work around the system. If we had to wait as long as our patients, perhaps we might be more enthusiastic about changing and leading the change that must happen in our systems. A recent report suggests that our ability to circumvent the system, at least in the US is associated with a higher prevalence of disease than would be expected in the population; in other words does the ease of access imply an ease of diagnosis. Having had a recent experience of healthcare, it does appear to me that at least for doctors, other doctors may be more likely to test and treat.
Mirror, Mirror on the wall, who is the best of us all?
Conventional wisdom suggest that bigger and more sophisticated hospitals offer the best care. However, my anecdotal experience suggest that this may not always be the case. There are some emerging data which also put the lie to this hypothesis. Just published is The Joint Commissions annual survey of hospital quality in the US.
The measures used to assess quality might be criticized as “process“ measures, i.e. Are we delivering the care that we are supposed to deliver? but these are basic widely agreed measures. The most stunning finding was that many of the big name hospitals, even those that have tried to make their name as institutions that prioritize quality and safe care do not feature. Or maybe not so surprising; in a culture in which individuals prize their autonomy, it will be easier for smaller hospitals to ensure they are consistent in applying processes.
The measures used to assess quality might be criticized as “process“ measures, i.e. Are we delivering the care that we are supposed to deliver? but these are basic widely agreed measures. The most stunning finding was that many of the big name hospitals, even those that have tried to make their name as institutions that prioritize quality and safe care do not feature. Or maybe not so surprising; in a culture in which individuals prize their autonomy, it will be easier for smaller hospitals to ensure they are consistent in applying processes.
Wednesday, September 7, 2011
Competition?
Competition is touted as a solution for all the ills that afflict healthcare, not withstanding the evidence from a market that is not deficient in competition, the US, that more competition does not equate to better healthcare. One of the great thinkers, Muir Gray, has written two recent blog posts, here and here, which outline a pragmatic framework which could be used to foster improved healthcare. Strongly recommended reading.
Systems Thinking in the Public Sector
I have previously written about Vanguard, John Seddon and his approach to systems thinking. His writing has been a revelation to me, plainly explaining how we can do things better with fewer resources, less waste, more customer satisfaction and more job satisfaction. Not quite a free lunch, but the next best thing. See the Amazon link on the side panel. I strongly recommend his books.
How to measure harm
Amongst the many challenges we face in trying to improve safety of care is the paucity of knowledge we possess about the rate and types of harm occurring to our patients. The traditional approach has been to identify sentinel cases, either because they are obvious or they are reported via traditional risk reporting structures. This approach has many limitations. A more recent approach has been to systematically review charts looking for evidence of adverse events, which allows one to both measure the rate of harm, identify areas of greatest risk and then one can determine whether changes made are having any meaningful effect in reducing rates of harm.
A paper just published (free here) describes an alternative approach in which a trained observer directly measures rates and type of harm occurring. The authors found almost 14% of patients suffered at least one adverse event, and 6% of all patients suffered a preventable adverse event. Overall 33% of adverse events were judged to be preventable. The rate of harm varied widely by specialty with <2% of obstetric patients being harmed to 11% of medical and ICU patients being harmed. The severity of harm also varied, with almost 5% of cardiac ICU patients dying or being permanently disabled due to an AE.
A paper just published (free here) describes an alternative approach in which a trained observer directly measures rates and type of harm occurring. The authors found almost 14% of patients suffered at least one adverse event, and 6% of all patients suffered a preventable adverse event. Overall 33% of adverse events were judged to be preventable. The rate of harm varied widely by specialty with <2% of obstetric patients being harmed to 11% of medical and ICU patients being harmed. The severity of harm also varied, with almost 5% of cardiac ICU patients dying or being permanently disabled due to an AE.
Autumn and patient safety
After a long summer break, back to posting. I would strongly recommend this blog, authored by an Emergency Medicine physician, with a greta deal of expertise in the area of healthcare informatics. Well worth a read. http://frectal.com/
Friday, July 15, 2011
Systems Thinking in healthcare
This blog just launched is well worth checking out. Based on work by Vanguard, a UK systems thinking consultancy and its CEO, John Seddon. Seddons stuff, books, papers, podcasts etc are worth checking out. There is a simplicity which hides a very deep and profound complexity in his methods. I don't think they have done much in healthcare, but read Systems Thinking in the Public Sector , and you will immediately see analogies. Value Demand and Failure Demand have become part of my vernacular. Bottom line message, our healthcare system is broken, and we need to rethink it. Positive spin, there is a huge amount of waste. Read it and decide.
Thursday, July 14, 2011
Cowboys and Pit Crews
A great piece, as usual, from Gawande, with the aforementioned title. Bottom line, we have to change the way we think and work.
Tuesday, April 26, 2011

Sunday, April 24, 2011

Saturday, April 23, 2011

Thursday, April 21, 2011
Recession and Physical Child Abuse
A paper was presneted last week at the American Association of Neurological Surgeons' annual meeting in Denver by a fourth year medical student. Mary Huang presented her study which sought to determine whether there was an association between economic downturn and abusive head trauma in children. She found that the risk of abusive head trauma doubled during a economic recession, and the severity of the injuries appeared to increase also.
Wednesday, April 20, 2011
Patient Driven Care
A greta post on Paul Levys blog, in which he proclaims following a meeting in IHI that he is no longer an advocate for patient centered care, but henceforth will be proclaiming the benefits of patient driven care. In his own words,
"What I am suggesting is that clinicians should do their best to collaborate with patients to understand their needs and desires and to jointly design plans of care that are as consistent as possible with those needs and desires."
Such a move would require a sea change in the way we practice and deliver care. It reminds me of a good friend who when i told him the difficulty I was having in getting a computer in my clinic room asked me why I needed a computer. To access UpToDate and other resources, I replied. "You mean you would look up information in front of patients?", was the stunned response.
Pauls point aligns nicely with what Maureen Bisognano said at the International Forum, that patients are our greatest unused resource.
Sunday, April 17, 2011
Disclosure and Litigation
We are all aware of the reputation of the US legal system as litigation central for mistakes in healthcare. Surely the worst thing to do is to publicize ones mistakes in this environment? Paul Levy on his blog points out a fascinating cultural dichotomy. He explains how during his tenure as CEO of BIDMC, medical errors were publicized. He contrasts this openness with the reluctance of various European hospitals to disclose their errors. Perhaps we should be learning from our American cousins?
Lessons Learned
Just finished a book by a number of clinicians, all US based. It is outstanding. Written to honor Paul Batalden, it is a treasure chest of advice, hints, tips, aphorisms, about the practicalities of changing healthcare. Unusually I am unable to pick out a highlight, as the quality (no surprise) is uniformly excellent. Get it here.
Thursday, April 14, 2011
A vision of the future? Bilingual healthcare workers
From the inestimable Muir Gray, (thanks Tony), one possible approach to the problems facing us. Remember Einsteins definition of insanity, doing the same thing over and over and expecting different results. I think that summarizes healthcare. The model we have is designed, or rather evolved from the post war period to deal with a different set of problems. Acute self limited, or fatal illness. Coincident with the rise in healthcare technology, probably the early 50's with the development of ICUs following polio epidemics, the healthcare-industrial complex has in part generated problems and expectations that we are no longer equipped to handle. The paradigm of how care is delivered has to change radically. There is a very interesting book published in the 80's looking at how complex societies fail. The thesis and it applies equally well to complex systems is that a system evolves to deal with a complex problem, problems become more complex, hence the system becomes more complex and eventually a point of diminishing returns is reached where the inputs (think regulation, accreditation, legislation etc) consume more resources and the system collapses.
Gray provides one possible approach to this challenge. Basically the bilingualism to which he refers is that healthcare workers must be versed in not only the ability to provide clinical care to their patients,
"They need to know how to:
Gray provides one possible approach to this challenge. Basically the bilingualism to which he refers is that healthcare workers must be versed in not only the ability to provide clinical care to their patients,
"They need to know how to:
- Develop systems
- Build networks of clinicians and patients
- Design pathways
- Manage knowledge
- Harness the internet’s potential
- Engage patients
- Create and manage programme budgets
- Develop the right culture"
He describes this as population medicine. It is highly recommended.
Much ado about bundles
Following yesterdays post about bundles, a couple of interesting papers from this weeks NEJM. Two studies here and here, and an editorial about reducing infection in hospitals. The two studies came to different conclusions; the first examined the efficacy of screening for MRSA in ICUs and implementing barrier precautions on all patients until their MRSA status was known. The interventions were not shown to be effective in reducing transmission of MRSA or VRE. However, and this is the really big take home message for me, in cases where hand hygeine or glovers were indicated, the compliance with these measures was as low as 62%!
In contrast, the VA study instituted a bundle approach; a MRSA bundle was instituted in 2007 and over 2 million hospital discharges were studied. The rate of health care associated MRSA infections fell by between 45% (outside ICU) and 62% (inside ICU) over a two year period.
For some expert comment, see this CDC post.
In contrast, the VA study instituted a bundle approach; a MRSA bundle was instituted in 2007 and over 2 million hospital discharges were studied. The rate of health care associated MRSA infections fell by between 45% (outside ICU) and 62% (inside ICU) over a two year period.
For some expert comment, see this CDC post.
Is it better to be a dog or a medical student?
Lots doom and gloom out there, so something to put a smile on your face, unless you are a med student!
From A cartoon guide to becoming a doctor.

From A cartoon guide to becoming a doctor.
Wednesday, April 13, 2011
Health care spend, any room to reduce it?
While not strictly looking at quality and cost at a hospital level, a paper just published by OECD examines the potential for savings in health expenditure. It suggest that countries can achieve savings up to 5% of GNP by all countries becoming as efficient as the best performing countries. Note that there does not appear to be much if any correlation between healthcare spend and outcomes across countries. The authors suggest that countries by reaching the level of the best performers would increase life expectancy at birth by two years; in contrast a 10% rise in health expenditure would increase life expectancy by three to four months.
Harm
Great discussion by Bob Wachter on his blog about harm, preventable harm, errors and trigger tools amongst other things. He makes the point that we should focus on eliminating preventable harm, at least in the first instance. Beth Israel Deaconess publishes on its public website details on its progress towards eliminating preventable harm.
Giving doctors orders
If you are a doc, you know that very few people order you around, apart form your kids. Maureen Dowd discusses this and its implications in todays NYT. Yet another story of a family member dying. But she can be very amusing, and this is one of her funnier and more poignant pieces.
Bundles of joy or of sorrow?
The idea of bundles makes intuitive sense, gather together some evidence based interventions and ensure they are implemented reliably all the time, sit back and watch the magic. Pronovost showed the power of bundles in his NEJM paper some years ago. An observational study by Jarman and others in the BMJ last year suggested that using various bundles in a large London hospital was associated with a large reduction in hospital mortality.
So along come the surgeons to upset the consensus. A study in Archives of Surgery compared standard institutional practice with an extended bundle of interventions, all of which had been previously demonstrated in isolation to be effective. These interventions included:
So along come the surgeons to upset the consensus. A study in Archives of Surgery compared standard institutional practice with an extended bundle of interventions, all of which had been previously demonstrated in isolation to be effective. These interventions included:
- No pre-operative bowel preparation
- Pre-operative and intra-operative patient warming
- Supplemental oxygen intra and post operatively
- Intra-operative fluid restriction
- Use of a surgical wound protector
Any explanation? Its possible that the interventions are ineffective, or less likely that they are counter synergistic, i.e. although singly beneficial, when combined they counteract one another. Alternatively even positive studies may due to chance be negative. The main concern though apart from giving ammunition to those who wish to reject the benefits of standardisation is that there will be a call for more RCTs in this and every other areas. While we have traditionally believed that RCTs are the gold standard, Ioanniddis work is even questioning this dictum. The other big problem in conducting RCTs is that we assume that apart from the intervention being studied, all other factors are uniform. This is clearly not the case, and this has proven to be a difficult obstacle to surmount in trials of equipment such as new ventilators.
Game changing move for patient safety in US
Bob Wachter on THCB has a piece on what he calls a game changing safety initiative. Berwick and Kathleen Sibelius announced yesterday the "Partnership for Patients". This is a very ambitious well funded widely supported program. Its stated goals are to reduce preventable harm in US hospitals by 40% and preventable readmissions by 20% by 2013! It's nice to see Berwick has not lost his taste for aiming high. To quote Wachter:
Interestingly, the means of audit to confirm compliance with these aims will be a detailed chart which appears to me to be using the IHI global trigger tool. Exciting times.
It would appear in some ways to be modeled on the 100,000 Lives campaign in that it sets lofty goals, appeals to sentiment, has a short time frame and uses social pressure to ensure others want to join.
The financial stick is that by 2015, 9% of medicare reimbursement will be tied to reaching these goals.
- "For the first time, it establishes safety goals and programs as a private/public partnership, with early buy in from large insurers and employers. A broad tableau of leaders from provider organizations, insurers, federal agencies, businesses, and patient groups shared the stage with Sebelius and Berwick at this morning’s announcement to highlight the partnership theme.
- It provides large amounts of funding and technical assistance – nearly one billion dollars – both through the new CMS Innovation Center and elsewhere, to promote new knowledge and skill building.
- Like the 100K Lives Campaign, it seeks commitments from hospital executives and boards to tackle key safety goals.
- It provides support for collaborative networks designed to promote shared learning.
- It rewards hospitals for achieving certain milestones with both recognition and additional resources; those that do very well will be eligible to receive funding to help other hospitals improve."
Interestingly, the means of audit to confirm compliance with these aims will be a detailed chart which appears to me to be using the IHI global trigger tool. Exciting times.
It would appear in some ways to be modeled on the 100,000 Lives campaign in that it sets lofty goals, appeals to sentiment, has a short time frame and uses social pressure to ensure others want to join.
Tuesday, April 12, 2011
Innovation
A quote that came through in an IHI email today about innovation:
"Innovation distinguishes between a leader and a follower"
Steve Jobs
Not sure I totally agree. Many innovators failed to benefit from their innovations, and often the mindset of an innovator is antithetical to being a leader. Nevertheless, a great quote from the man who invented Peters iPad 2, (x2)
"Innovation distinguishes between a leader and a follower"
Steve Jobs
Not sure I totally agree. Many innovators failed to benefit from their innovations, and often the mindset of an innovator is antithetical to being a leader. Nevertheless, a great quote from the man who invented Peters iPad 2, (x2)
Depression, the inside story
Anyone interested in how our system within our own lifetimes treated people should read this article. It is harrowing. Unfortunately I think mental illness is still seen as a weakness, "just snap out of it, for gods sake" is often the response. I am aware of employers who have failed in their statutory responsibility to ensure those with mental illness receive the same entitlements and protections afforded to every employee. We are not as civilized as we think.
A quote from the psychiatrist who treated the patient:
A quote from the psychiatrist who treated the patient:
"Our patients are our best teachers. Jackie has taught me a huge amount about depression: what it feels like, the impact on sufferers’ and their family, and what does and doesn’t help.I have seen the toll taken by this ubiquitous disease, no less devastating in its impact than other chronic conditions. Jackie, an able and enthusiastic student, could barely finish her course at University, her employment prospects have been blighted, her social life restricted, and her capacity for pleasure and fulfilment curtailed. At their worst psychiatric services reinforce sufferers’ feelings of isolation and powerlessness."
Increase comfort in the face of uncertainty
IDEO are a very interesting design and innovation firm based in California, and have done a lot of work in this area with Kaiser Permanante. They have provided assistance to the NHS Institute for Innovation and Improvement, Texas Children's Paediatric Associates, (the largest primary paediatric care network in the US) and many others. Their website is well worth checking out for anyone with an interest in healthcare innovation in its softer (i.e. not hardware, expensive drugs and hi tech equipment) guise. What caught my eye recently was a blog by an IDEO employee with the title that I have posted above. I liked their use of data from Twitter, and Google Analytics to measure the "buzz" in real time generated by their ideas.
This comes back to the point made by Maureen Bisognano recently, about using the power of patients to seek ideas. If we could measure what people believe is important judged by what they search or discuss on line, perhaps it might help us focus on what matters to patients as opposed to what matters to the "providers". Just a thought.
This I think is an area where some Irish design consultancies might find a niche.
This comes back to the point made by Maureen Bisognano recently, about using the power of patients to seek ideas. If we could measure what people believe is important judged by what they search or discuss on line, perhaps it might help us focus on what matters to patients as opposed to what matters to the "providers". Just a thought.
This I think is an area where some Irish design consultancies might find a niche.
Monday, April 11, 2011

Global Trigger Tools
Thanks to Annette and Levette. Two important pieces to check out if you are interested in trigger tools. First a paper in Health Affairs showing that the use of the Global Trigger Tool detects adverse events at a rate 10 times greater than voluntary reporting or using the AHRQ patient safety indicators.
Second, an upcoming WIHI:
The Power to Detect and Improve: Revisiting the IHI Global Trigger Tool and Adverse Events
Thursday, April 14, 2011, 7pm MT. See here for details. Both are free. The WIHI features great faculty. Check it out.
Second, an upcoming WIHI:
The Power to Detect and Improve: Revisiting the IHI Global Trigger Tool and Adverse Events
Thursday, April 14, 2011, 7pm MT. See here for details. Both are free. The WIHI features great faculty. Check it out.
Mental illness and children
A great image showing the extent of psychoactive drug prescribing in the US. While there are many
interesting explanations for such rampant pharmaco-terrorism, this post has another purpose.
 A recent story caught my eye, in fact it was so striking it kidnapped my brain. Headlined, "Is that Thorazine in the babies bottle?", it discussed the relentless rise in diagnosing and treating psychiatric illness in chilren and infants. According to the story, 500,000 children in the US are prescribed anti-psychotics! When I went looking for data about the incidence/ prevalence of psychiatric illness in children, the numbers are mind boggling. According to childstats.gov, in 2008 8% of children aged 12-17 experienced a major depressive episode. Of course, some may question this data, but it does appear that the incidence of major psychiatric illness, especially depression is rising across the Western world, and it has been suggested that the major contributor to this increase is rising economic and social inequality. If this is the case, medicating children from a very young age is not the solution, and is really only addressing the symptoms of a societal problem. For a more detailed discussion, read The Spirit Level . This is a magnificent book, likely to be seen in 50 years as the seminal public health work.
A recent story caught my eye, in fact it was so striking it kidnapped my brain. Headlined, "Is that Thorazine in the babies bottle?", it discussed the relentless rise in diagnosing and treating psychiatric illness in chilren and infants. According to the story, 500,000 children in the US are prescribed anti-psychotics! When I went looking for data about the incidence/ prevalence of psychiatric illness in children, the numbers are mind boggling. According to childstats.gov, in 2008 8% of children aged 12-17 experienced a major depressive episode. Of course, some may question this data, but it does appear that the incidence of major psychiatric illness, especially depression is rising across the Western world, and it has been suggested that the major contributor to this increase is rising economic and social inequality. If this is the case, medicating children from a very young age is not the solution, and is really only addressing the symptoms of a societal problem. For a more detailed discussion, read The Spirit Level . This is a magnificent book, likely to be seen in 50 years as the seminal public health work.
interesting explanations for such rampant pharmaco-terrorism, this post has another purpose.
Saturday, April 9, 2011
Friday, April 8, 2011
International Forum and Social Movements
Helen Bevan and Maxine Power gave a wonderful hour long talk on the power of social movements, mobilising weak network connections, (in contrast to the network effects we usually think of being most powerful such as family, peers) in generating will to change. The focus was hospital based care, but I wonder how soon we will begin to see such strategies applied to the overwhelming need for society to concentrate on health and prevention.
Thursday, April 7, 2011

{kind=link}
Forum; motivation and morale
Both Maureen Bisognano and Helen Bevan referenced the need to capture ant tap resources that we traditionally have failed to recognise. In Maureens case, the patient is a huge resource; Helen argues that we fail to capture the intrinsic motivation of many employees. The idea is that if an organisation can tap this, productivity can increase 30-40%.
Subscribe to:
Posts (Atom)